

Combing stereotactic body radiotherapy with checkpoint inhibitors after oligoprogression in advanced non-small cell lung cancer
- PMID: 35070747
- PMCID: PMC8743519
- DOI: 10.21037/tlcr-21-682
Combing stereotactic body radiotherapy with checkpoint inhibitors after oligoprogression in advanced non-small cell lung cancer
Erratum in
-
Erratum to combing stereotactic body radiotherapy with checkpoint inhibitors after oligoprogression in advanced non-small cell lung cancer.Transl Lung Cancer Res. 2022 Mar;11(3):504-505. doi: 10.21037/tlcr-2022-1. Transl Lung Cancer Res. 2022. PMID: 35399569 Free PMC article.
Abstract
Background: Immunotherapy has brought substantial benefit for patients with advanced non-small cell lung cancer (NSCLC); however, resistance may occur, of which oligoprogression is most common. There are no standard strategies to overcome acquired resistance, thus exploring potential effective approaches is critical. Our study evaluated the clinical outcome of combing stereotactic body radiotherapy (SBRT) with checkpoint inhibitors (CPIs) in oligoprogressive NSCLC.
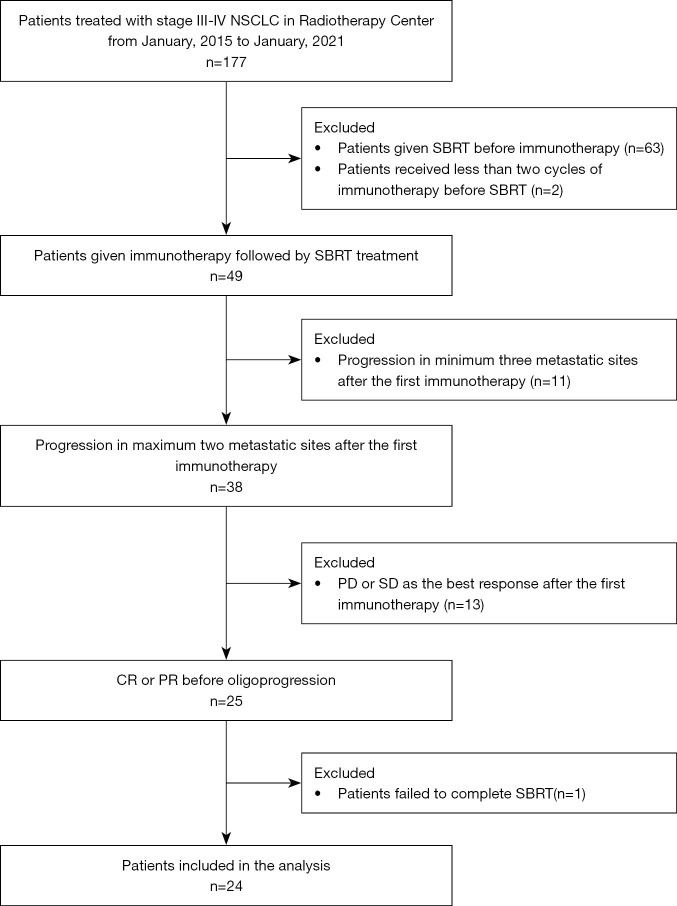
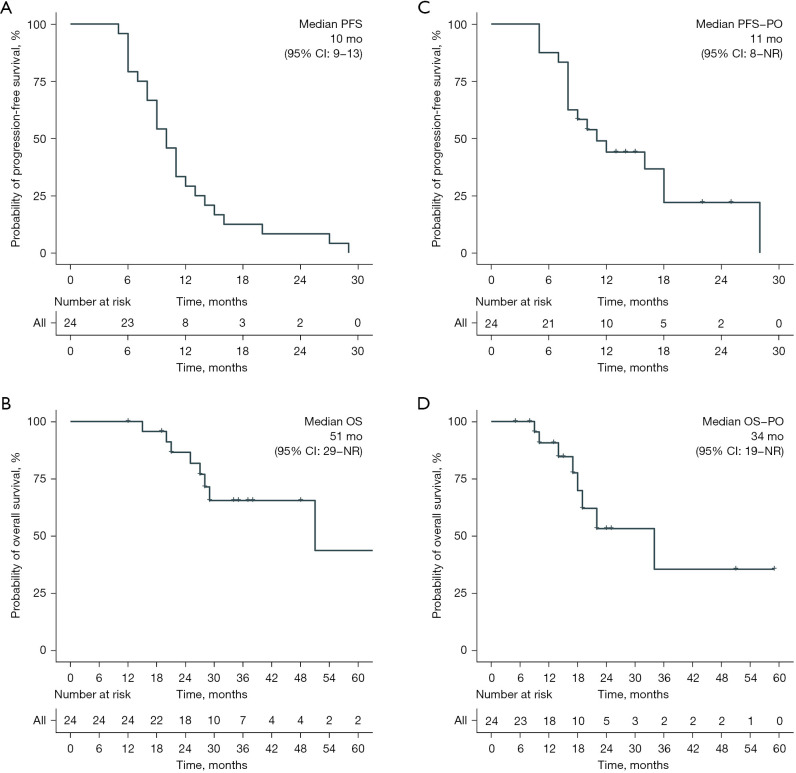
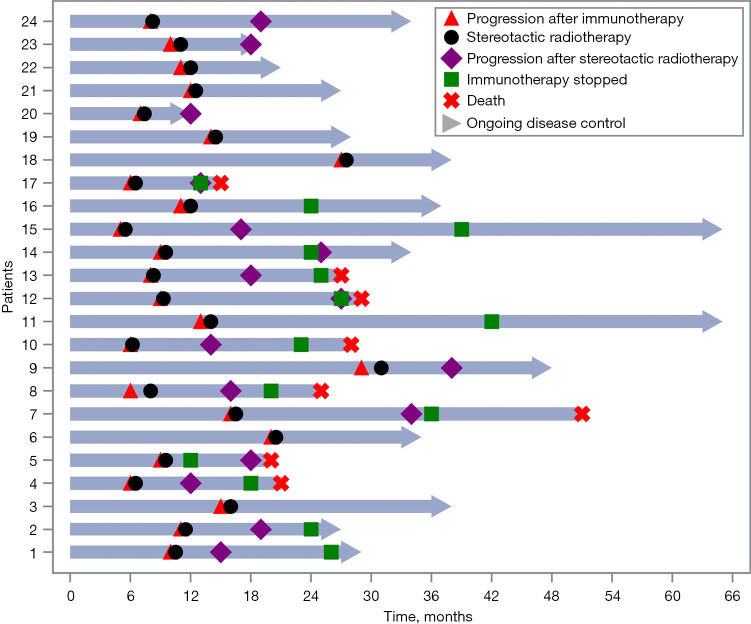
Methods: We retrospectively reviewed patients with advanced NSCLC who received SBRT for oligoprogressive lesions after acquired resistance to CPIs in our hospital between January 2015 and January 2021. Acquired resistance was defined as initial complete/partial response (CR/PR) followed by progression/death. Oligo patterns of acquired resistance were defined as progression in ≤2 sites of disease. We evaluated the local control rate (LR), progression-free survival (PFS-PO), overall survival (OS-PO), and safety of combing SBRT after oligoprogression.
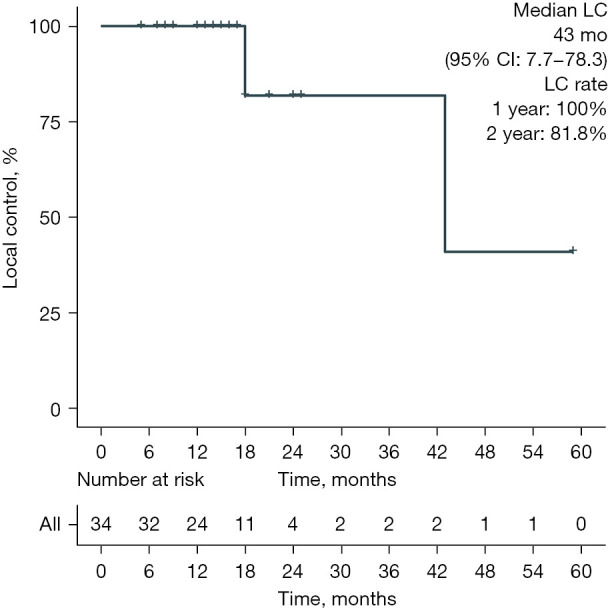
Results: Among 177 patients reviewed, 24 patients were included. Fifteen (62.5%) were diagnosed with adenocarcinoma, and 20 (83.3%) were with stage IV. Before oligoprogression, immunotherapy was used as first-line treatment in 16 (66.7%) patients, and 4 (16.7%) received monotherapy. After combing SBRT with CPIs, the median PFS-PO and OS-PO were 11 months (95% CI: 8-NA) and 34 months (95% CI: 19-NA). The median LC of 34 oligoprogressed lesions was 43 months (95% CI: 7.7-78.3). The 1- and 2-year LC rates were 100% and 81.8%, respectively. Patients with adenocarcinoma, lung immune prognostic index (LIPI) (≥1), and positive PD-L1 tended to achieve favorable survival benefits.
Conclusions: We observed considerable benefit of local control and survival by combing SBRT in patients with oligoprogression after required resistance to CPIs in NSCLC. The adverse events are well managed. Our results suggest that combing SBRT with CPIs could be a potential strategy to overcome acquired resistance.
Keywords: Non-small cell lung cancer (NSCLC); checkpoint Inhibitor (CPI); oligoprogression; stereotactic body radiotherapy (SBRT); survival.
2021 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/tlcr-21-682). Yong Song serves as an Editor-in-Chief of Translational Lung Cancer Research. The other authors have no conflicts of interest to declare.
Figures
References
-
- Schoenfeld AJ, Rizvi H, Memon D, et al. Acquired resistance to PD-1 blockade in NSCLC. J Clin Oncol 2020;38:9621. 10.1200/JCO.2020.38.15_suppl.9621 - DOI
LinkOut - more resources
Full Text Sources
Research Materials