

Primary adrenal tuberculosis infection in patients with Behcet's disease presenting as isolated adrenal metastasis by 18F-FDG PET/CT: a rare case report and literature review
- PMID: 35070903
- PMCID: PMC8749099
- DOI: 10.21037/gs-21-511
Primary adrenal tuberculosis infection in patients with Behcet's disease presenting as isolated adrenal metastasis by 18F-FDG PET/CT: a rare case report and literature review
Abstract
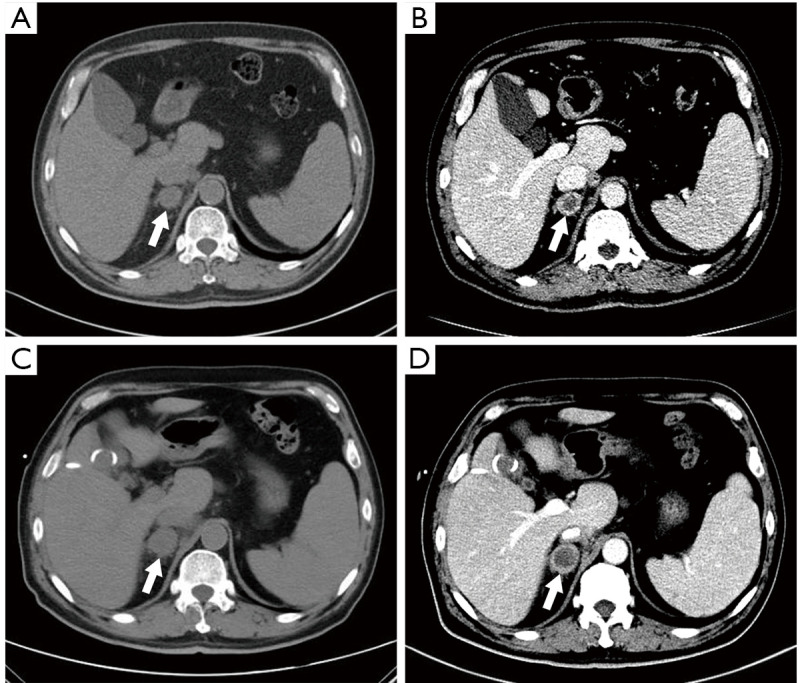
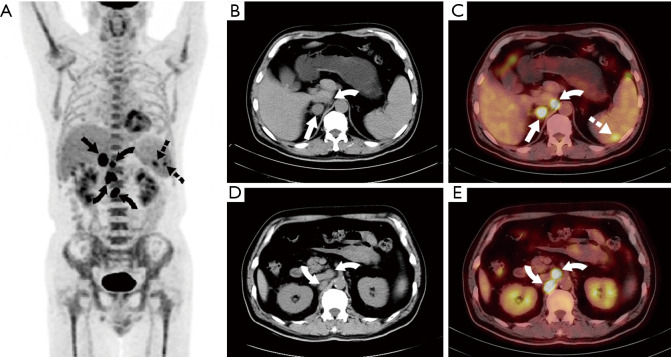
Primary adrenal tuberculosis (TB) is a rare type of extrapulmonary tuberculosis (EPTB). A pathological biopsy is usually required to make a definite diagnosis due to nonspecific symptoms. Antituberculous chemotherapy is the main treatment regimen, and cortisol replacement therapy should be added when adrenal insufficiency is involved. Here, we present a 59-year-old man who had recurrence of oral and genital aphthosis for 3 years and was diagnosed with Behcet's disease (BD), which was cured by thalidomide. After 10 days of admission, the patient had sudden abdominal pain in the right upper quadrant with high fever and was diagnosed with acute cholecystitis attack, which was treated by percutaneous transhepatic gallbladder drainage (PTGBD). Further contrast-enhanced CT showed a right adrenal mass with a diameter of 2.0 cm, and PET-CT indicated intense 18F-fluorodeoxyglucose (18F-FDG) uptake in the right adrenal mass with a maximum standardized uptake value (SUVmax) of 15.2. As a metastatic adrenal mass was suspected, the patient underwent retroperitoneal laparoscopic adrenalectomy. Histopathological and immunohistochemical analysis revealed primary adrenal TB. After routine anti-tuberculosis treatment with isoniazid, rifampin, pyrazinamide and ethambutol for six months, the patient was cured and discharged. In summary, primary unilateral adrenal TB without adrenal insufficiency is difficult to diagnose only on the basis of clinical manifestations and examinations. Further studies are needed to develop an easier and more accurate diagnostic examination.
Keywords: Behcet’s disease; PET/CT; Primary adrenal tuberculosis; adrenal metastatic mass; case report.
2021 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/gs-21-511). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Ulcerative intestinal tuberculosis case as a complication of treatment by infliximab for intestinal Behçet's disease: A case report.Medicine (Baltimore). 2019 Oct;98(43):e17652. doi: 10.1097/MD.0000000000017652. Medicine (Baltimore). 2019. PMID: 31651888 Free PMC article.
-
Sequential 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET) scan findings in patients with extrapulmonary tuberculosis during the course of treatment-a prospective observational study.Eur J Nucl Med Mol Imaging. 2020 Dec;47(13):3118-3129. doi: 10.1007/s00259-020-04888-7. Epub 2020 Jun 2. Eur J Nucl Med Mol Imaging. 2020. PMID: 32483653
-
Primary adrenal non-Hodgkin lymphoma: a case report and review of the literature.J Med Case Rep. 2017 Apr 15;11(1):108. doi: 10.1186/s13256-017-1271-x. J Med Case Rep. 2017. PMID: 28410600 Free PMC article. Review.
-
Advances in imaging of tuberculosis: the role of ¹⁸F-FDG PET and PET/CT.Curr Opin Pulm Med. 2014 May;20(3):287-93. doi: 10.1097/MCP.0000000000000043. Curr Opin Pulm Med. 2014. PMID: 24614238 Review.
Cited by
-
Adrenal Abscesses: A Systematic Review of the Literature.J Clin Med. 2023 Jul 11;12(14):4601. doi: 10.3390/jcm12144601. J Clin Med. 2023. PMID: 37510716 Free PMC article. Review.
-
Complete recovery after glucocorticoid replacement therapy in a case of primary adrenal insufficiency caused by adrenal tuberculosis infection.Endocrinol Diabetes Metab Case Rep. 2023 Dec 13;2023(4):23-0112. doi: 10.1530/EDM-23-0112. Print 2023 Oct 1. Endocrinol Diabetes Metab Case Rep. 2023. PMID: 38088358 Free PMC article.
-
Advances in multimodal imaging for adrenal gland disorders: integrating CT, MRI, and nuclear medicine.Jpn J Radiol. 2025 Jun;43(6):903-926. doi: 10.1007/s11604-025-01732-6. Epub 2025 Jan 11. Jpn J Radiol. 2025. PMID: 39794659 Free PMC article. Review.
References
-
- Addison T. A Collection of the published writings of the late Thomas Addison, MD. 1868.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials