

Significance of Lymph Node Metastasis in the Treatment of Gastric Cancer and Current Challenges in Determining the Extent of Metastasis
- PMID: 35071010
- PMCID: PMC8777129
- DOI: 10.3389/fonc.2021.806162
Significance of Lymph Node Metastasis in the Treatment of Gastric Cancer and Current Challenges in Determining the Extent of Metastasis
Abstract
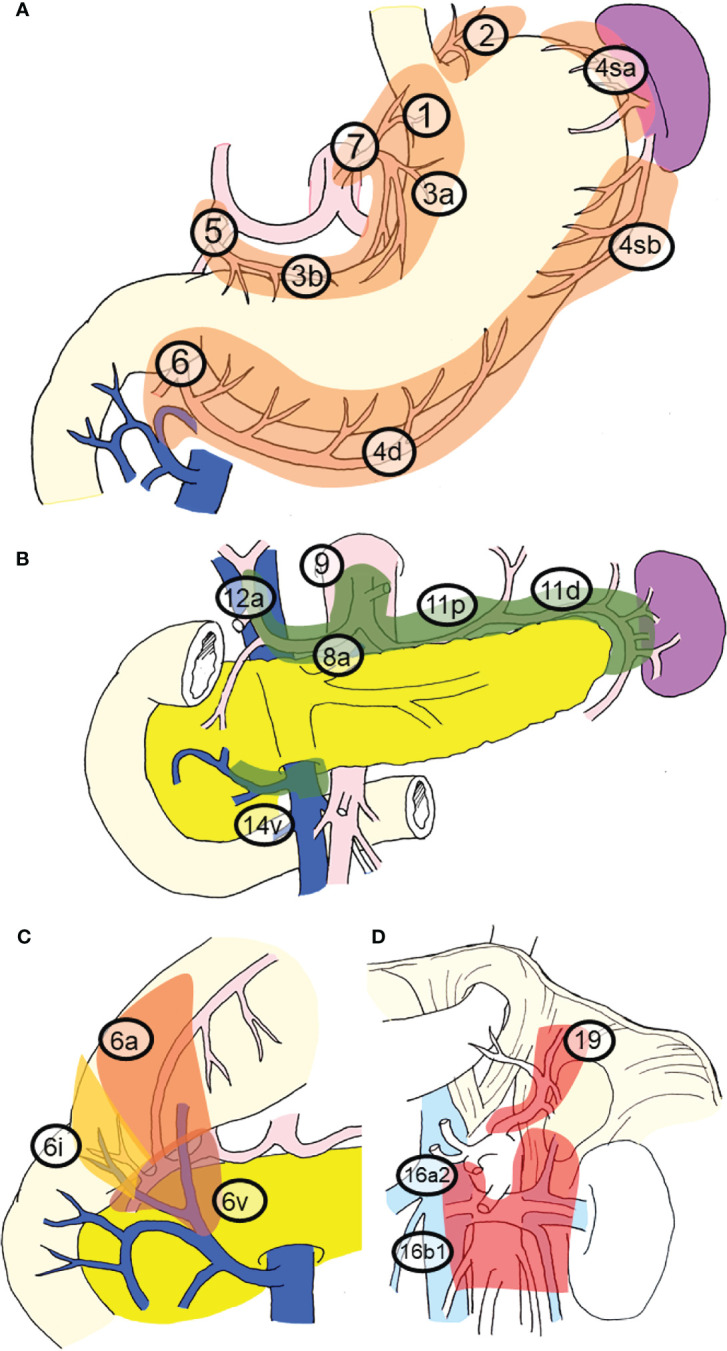
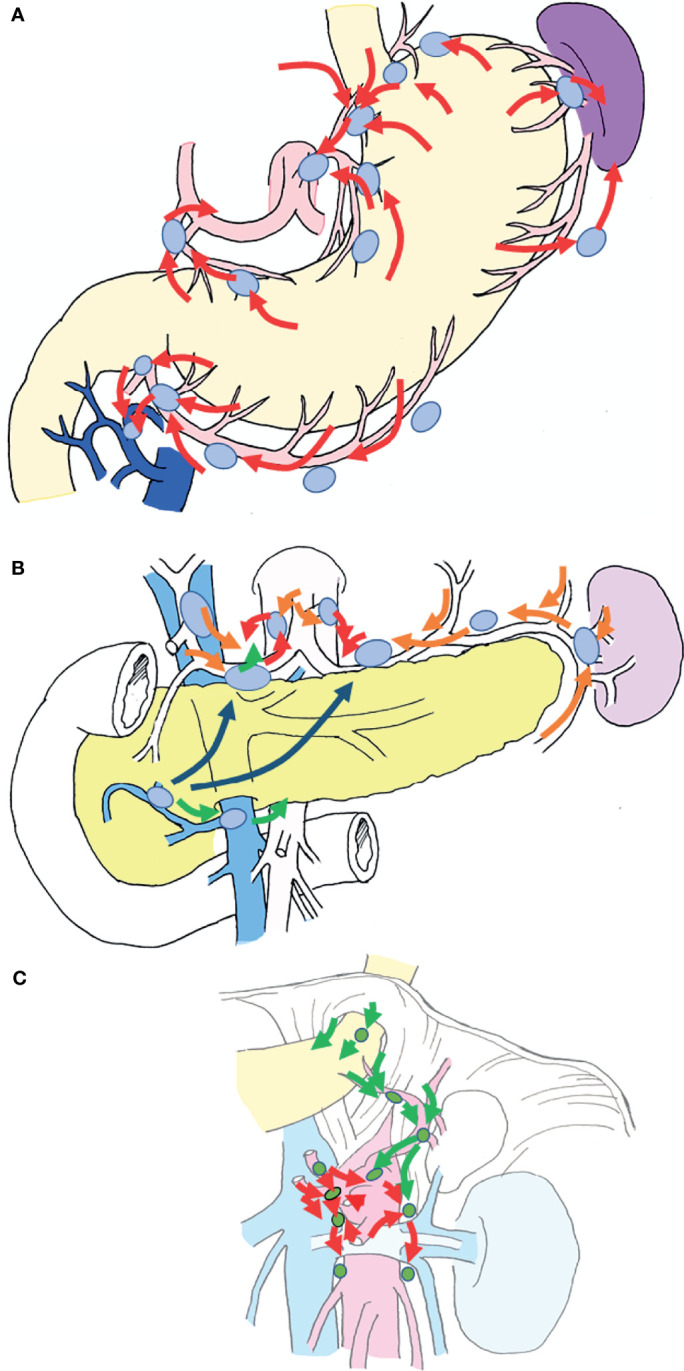
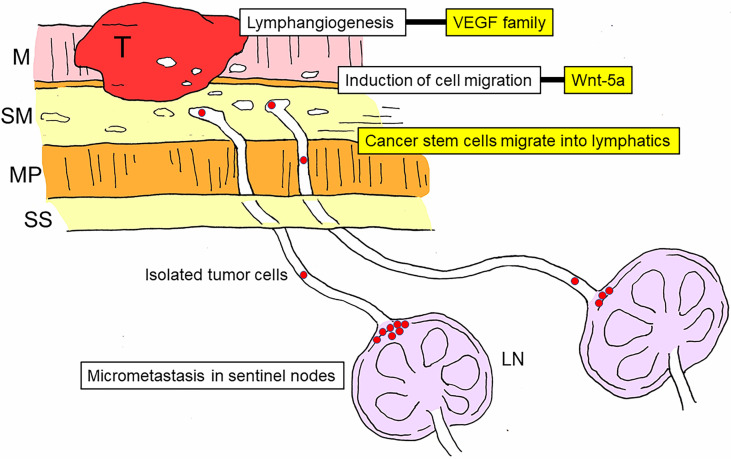
The stomach exhibits abundant lymphatic flow, and metastasis to lymph nodes is common. In the case of gastric cancer, there is a regularity to the spread of lymph node metastasis, and it does not easily metastasize outside the regional nodes. Furthermore, when its extent is limited, nodal metastasis of gastric cancer can be cured by appropriate lymph node dissection. Therefore, identifying and determining the extent of lymph node metastasis is important for ensuring accurate diagnosis and appropriate surgical treatment in patients with gastric cancer. However, precise detection of lymph node metastasis remains difficult. Most nodal metastases in gastric cancer are microscopic metastases, which often occur in small-sized lymph nodes, and are thus difficult to diagnose both preoperatively and intraoperatively. Preoperative nodal diagnoses are mainly made using computed tomography, although the specificity of this method is low because it is mainly based on the size of the lymph node. Furthermore, peripheral nodal metastases cannot be palpated intraoperatively, nodal harvesting of resected specimens remains difficult, and the number of lymph nodes detected vary greatly depending on the skill of the technician. Based on these findings, gastrectomy with prophylactic lymph node dissection is considered the standard surgical procedure for gastric cancer. In contrast, several groups have examined the value of sentinel node biopsy for accurately evaluating nodal metastasis in patients with early gastric cancer, reporting high sensitivity and accuracy. Sentinel node biopsy is also important for individualizing and optimizing the extent of uniform prophylactic lymph node dissection and determining whether patients are indicated for function-preserving curative gastrectomy, which is superior in preventing post-gastrectomy symptoms and maintaining dietary habits. Notably, advancements in surgical treatment for early gastric cancer are expected to result in individualized surgical strategies with sentinel node biopsy. Chemotherapy for advanced gastric cancer has also progressed, and conversion gastrectomy can now be performed after downstaging, even in cases previously regarded as inoperable. In this review, we discuss the importance of determining lymph node metastasis in the treatment of gastric cancer, the associated difficulties, and the need to investigate strategies that can improve the diagnosis of lymph node metastasis.
Keywords: MDCT; gastric cancer; lymph node metastasis; sentinel node; staging.
Copyright © 2022 Kinami, Saito and Takamura.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Brierley J, Gospodarowicz M, Wittekind C. UICC TNM Classification of Malignant Tumours. 8th. Chichester: Wiley; (2017).
-
- Japanese Gastric Cancer Association . Japanese Classification of Gastric Carcinoma. 15th. Tokyo: Kanehara Shuppan; (2017). - PubMed
-
- Ronellenfitsch U, Schwarzbach M, Hofheinz R, Kienle P, Kieser M, Slanger TE, et al. Perioperative Chemo(Radio)Therapy Versus Primary Surgery for Resectable Adenocarcinoma of the Stomach, Gastroesophageal Junction, and Lower Esophagus. Cochrane Database Syst Rev (2013) 31(5):CD008107. doi: 10.1002/14651858.CD008107.pub2 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources