

Anterior Approach to the Cervical Spine: Elegance Lies in Its Simplicity
- PMID: 35071061
- PMCID: PMC8751502
- DOI: 10.4103/ajns.AJNS_313_20
Anterior Approach to the Cervical Spine: Elegance Lies in Its Simplicity
Abstract
Introduction: Since the landmark publication by Smith and Robinson, approaches to the cervical spine anteriorly have undergone many modifications and even additions. Nevertheless, at its core, the anterior approach remains an elegant and efficient approach to deal with majority of cervical spine pathologies including the degenerative cervical spine.
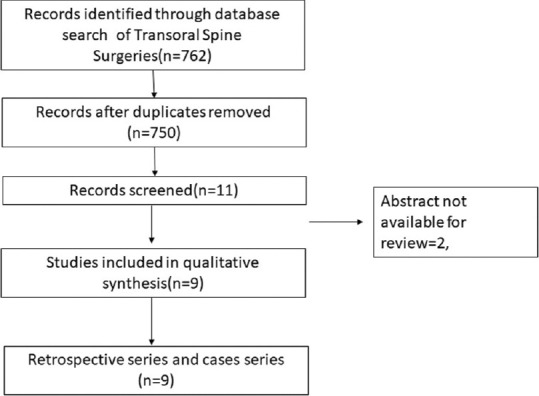
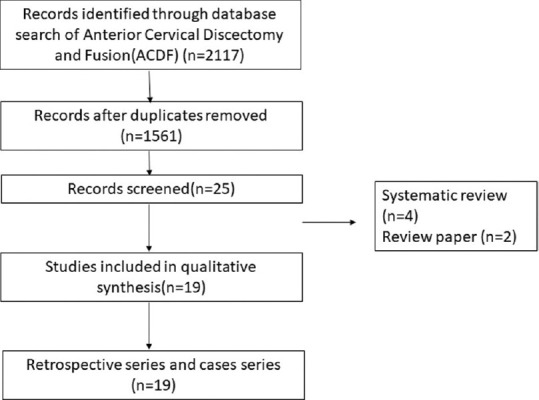
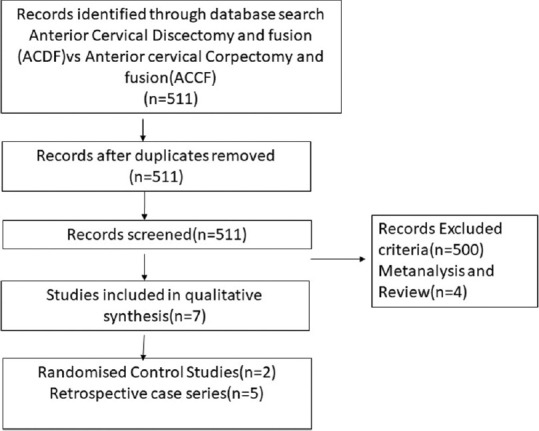
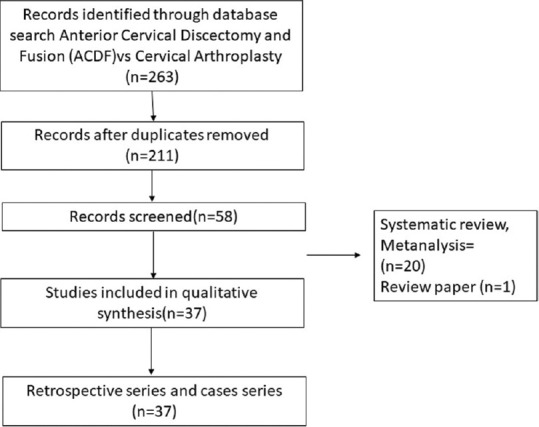
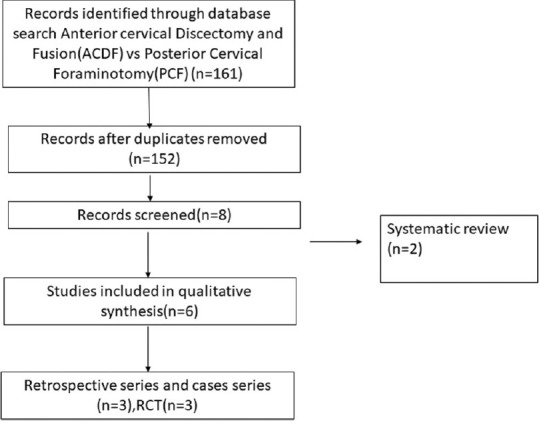
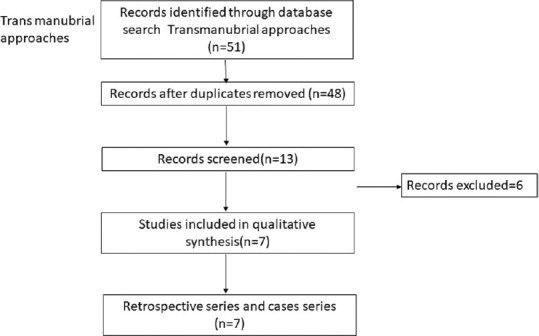
Methodology: For this review, we searched for all major cases series and randomized control trials of anterior cervical approaches using the PubMed databases. Articles having the details of clinical variables and outcomes were tabulated and analyzed.
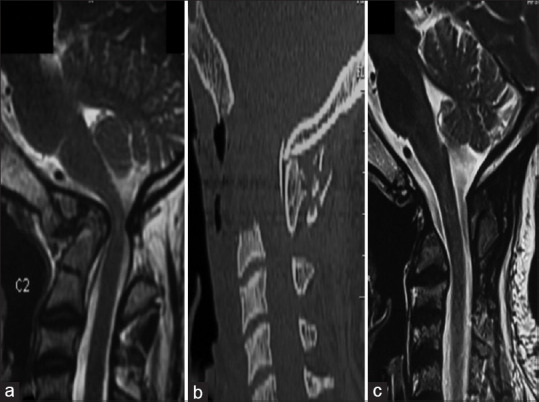
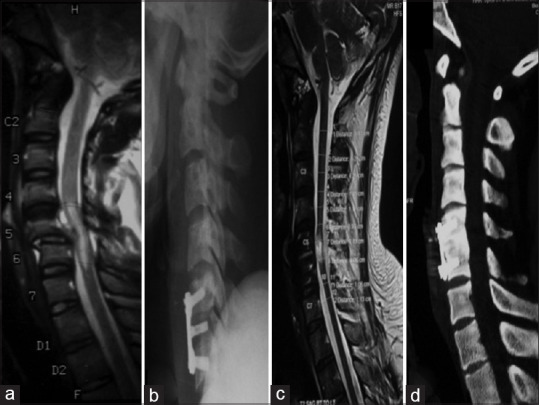
Results: A total of 9 case series for transoral, 7 case series for transmanubrial, 19 case series for anterior cervical discectomy and fusion (ACDF), 6 studies for ACDF versus posterior cervical foraminotomy, 37 case series for ACDF versus arthroplasty, and 7 studies for ACDF versus anterior cervical corpectomy and fusion have been included. The majority of the case series suggested that the anterior cervical procedures have good clinical outcomes. The upper cervical spine approached by the transoral route had good outcomes in ventral compressive pathologies, with morbidity of cerebrospinal fluid leak in 7% of patients. The midcervical spine approached by ACDF had better clinical outcomes equivalent to the majority of modifications even in multiple-level pathologies. The transsternal approach had provided greater access and stability to the cervicothoracic junction with minimal morbidity.
Conclusion: The anterior cervical approach can address the majority of cervical pathologies. They provide adequate corridor from craniovertebral junction to T4 with minimal morbidity, thus providing a good clinical outcome.
Keywords: Anterior cervical approach; cervical spine; cervical spondylotic myelopathy; corpectomy.
Copyright: © 2021 Asian Journal of Neurosurgery.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958;40-A:607–24. - PubMed
-
- Robinson RA, Southwick WO. Surgical approaches to the cervical spine. Instr Course Lect. 1960;17:299–330. - PubMed
-
- Bailey RW, Badgley CE. Stabilization of the cervical spine by anterior fusion. J Bone Joint Surg Am. 1960;42-A:565–94. - PubMed
-
- Naderi S, Alberstone CD, Rupp FW, Benzel EC, Baldwin NG. Cervical spondylotic myelopathy treated with corpectomy: Technique and results in 44 patients. Neurosurg Focus. 1996;1:e5. - PubMed
-
- Luk KD, Cheung KM, Leong JC. Anterior approach to the cervicothoracic junction by unilateral or bilateral manubriotomy. A report of five cases. J Bone Joint Surg Am. 2002;84:1013–7. - PubMed