

The Malawi emergency and critical care survey: A cross-sectional national facility assessment
- PMID: 35072017
- PMCID: PMC8762065
- DOI: 10.1016/j.eclinm.2021.101245
The Malawi emergency and critical care survey: A cross-sectional national facility assessment
Abstract
Background: Data on emergency and critical care (ECC) capacity in low-income countries (LICs) are needed to improve outcomes and make progress towards realizing the goal of Universal Health Coverage.
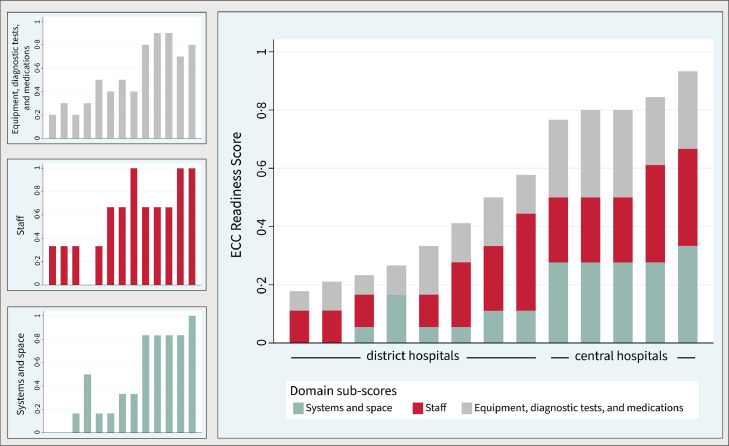
Methods: We developed a novel research instrument to assess public sector ECC capacity and service readiness in LICs. From January 20th to February 18th, 2020 we administered the instrument at all four central hospitals and a simple random sample of nine of 24 district hospitals in Malawi, a landlocked and predominantly rural LIC of 19·1 million people in Southern Africa. The instrument contained questions on the availability of key resources across three domains and was administered to hospital administrators and clinicians from outpatient departments, emergency departments, and inpatient units. Results were used to generate an ECC Readiness Score, with a possible range of 0 to 1, for each facility.
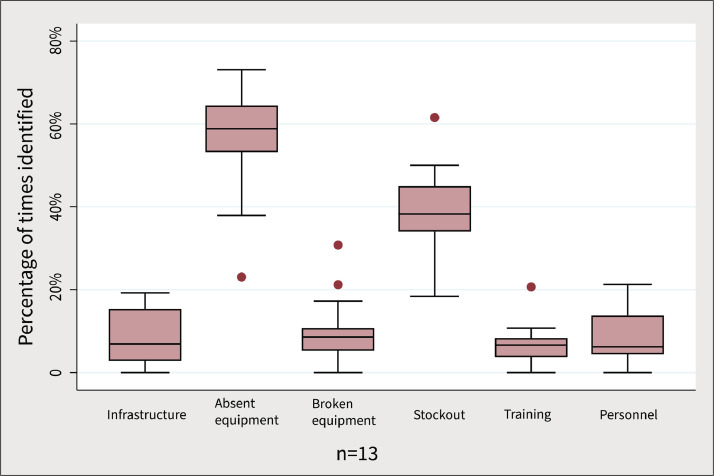
Findings: A total of 114 staff members across 13 hospitals completed interviews for this study. Three (33%) district hospitals and all four central hospitals had ECC Readiness Scores above 0·5 (p-value 0·070). Absent equipment was identified as the most common barrier to ECC Readiness. Central hospitals had higher median ECC Readiness Scores with less variability 0·82 (interquartile range: 0·80-0·89) than district hospitals (0·33, 0·23 to 0·50, p-value 0·021).
Interpretation: This is the first study to employ a systematic approach to assessing ECC capacity and service readiness at both district and central hospitals in Malawi and provides a framework for measuring ECC capacity in other LICs. Prior ECC assessments potentially overestimated equipment availability and our methodology may provide a more accurate approach. There is an urgent need for investments in ECC services, particularly at district hospitals which are more accessible to Malawi's predominantly rural population. These findings highlight the need for long-term investments in health systems strengthening and underscore the importance of understanding capacity in LIC settings to inform these efforts.
Funding: Division of Pulmonary and Critical Care Medicine, Brigham and Women's Hospital and Department of Emergency Medicine, Brigham and Women's Hospital.
Keywords: Emergency and critical care; Health systems strengthening; Intensive care; Malawi; Service readiness; Universal health coverage.
© 2022 The Authors.
Conflict of interest statement
PDS received support for this study from Brigham and Women's Hospital, Division of Pulmonary and Critical Care Medicine in the form of a faculty research fund and has received consulting fees from the University of California-San Francisco/Sustaining Technical and Analytic Resources as lead technical advisor for ventilator technical assistance in Haiti. SAR received support for this study in the form of a seed grant from Brigham and Women's Hospital Department of Emergency Medicine. JSM is the Chief Medical Officer at Partners In Health and sits on the boards of Village Health Works (Burundi/Muso and Mali), The Institute for Justice and Democracy in Haiti, and Free Speech for People.
Figures
References
-
- World Health Organization and the United Nations Children's Fund (UNICEF) World Health Organization; Geneva: 2018. A vision for primary health care in the 21st century: towards universal health coverage and the sustainable development goals.https://www.who.int/docs/default-source/primary-health/vision.pdf (accessed Sept 27, 2021)
-
- Firth P., Ttendo S. Intensive care in low-income countries–a critical need. N Engl J Med. 2012;367:1974–1976. - PubMed
-
- Murthy S., Adhikari N.K. Global health care of the critically ill in low-resource settings. Ann Am Thorac Soc. 2013;10:509–513. - PubMed
LinkOut - more resources
Full Text Sources
