

A Population-Based Study of Unexplained/Lone Atrial Fibrillation: Temporal Trends, Management, and Outcomes
- PMID: 35072029
- PMCID: PMC8767123
- DOI: 10.1016/j.cjco.2021.09.006
A Population-Based Study of Unexplained/Lone Atrial Fibrillation: Temporal Trends, Management, and Outcomes
Abstract
Background: Previous studies on lone/unexplained atrial fibrillation and atrial flutter (AF) did not exclude patients with contemporary secondary AF triggers. We characterized unexplained AF using a strict definition, and compared it to secondary AF.
Methods: In this population-based study, unexplained AF was defined by the lack of any identifiable triggering medical/surgical diagnosis. Comparisons by AF type (unexplained vs secondary), age-of-onset (≤ / > 65 years), and sex were undertaken. Data were acquired by linking 6 population databases maintained by the Alberta Ministry of Health over a 9-year period (April 2006 to March 2015). The primary composite outcome of stroke, transient ischemic attack, thromboembolism, and/or death was assessed.
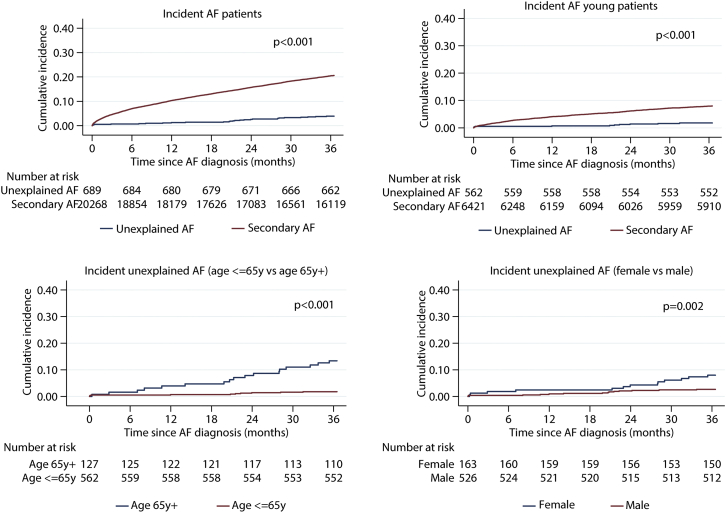
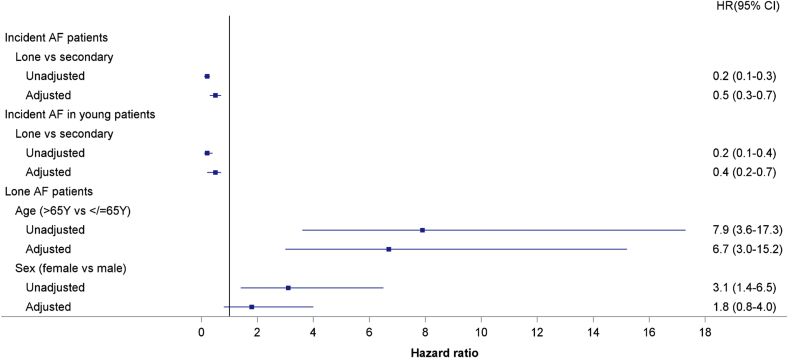
Results: There were 33,150 incident AF diagnoses identified, including 1145 patients (3.5%) with unexplained AF, 931 (81.2%) of whom were aged ≤ 65 years (2.8% of diagnoses, and 79% male). Patients with unexplained AF less often received rate/rhythm-control drugs (P < 0.0001), but they more often underwent electrical cardioversion (P < 0.0001) vs secondary AF patients. Men were younger at unexplained AF diagnosis (45 [interquartile range: 34-59] vs 58 [interquartile range: 40-69] years; P < 0.001). After adjusting for age at diagnosis, there were no sex-based differences in the primary outcome. Event-free survival in young unexplained AF (age ≤ 65 years) was 99.4% at 1 year and 98.3% at 3 years. At 3 years, hospitalization(s)/emergency visit(s) for noncardiovascular reasons and for AF occurred in 56.6% and 23.8% of these patients, respectively.
Conclusions: Using a strict contemporary definition of unexplained AF, this study shows that the condition is rare, predominantly male, and has excellent event-free survival. However, the high rate of acute hospital utilization after diagnosis is concerning.
Contexte: Les études précédentes sur le flutter auriculaire et la fibrillation auriculaire (FA) idiopathiques/inexpliqués n’excluaient pas les patients présentant des déclencheurs contemporains de FA secondaire. Nous avons caractérisé la FA inexpliquée en utilisant une définition stricte, et l’avons comparée à la FA secondaire.
Méthodologie: Dans cette étude basée sur une population, la FA inexpliquée a été définie par l’absence de tout diagnostic médical/chirurgical de déclencheur identifiable. Des comparaisons par type de FA (inexpliquée vs secondaire), par âge d’apparition (≤ / > 65 ans) et par sexe ont été effectuées. Les données ont été acquises en reliant six bases de données de population maintenues par le ministère de la Santé de l’Alberta sur une période de neuf ans (avril 2006 à mars 2015). Le paramètre d’évaluation principal comprenant l’accident vasculaire cérébral (AVC), l’accident ischémique transitoire, la thromboembolie et/ou le décès a été évalué.
Résultats: Au total, 33 150 diagnostics de FA ont été recensés, dont 1 145 patients (3,5 %) présentant une FA inexpliquée, parmi lesquels 931 (81,2 %) étaient âgés de ≤ 65 ans (2,8 % des diagnostics, et 79 % d’hommes). Les patients atteints de FA inexpliquée ont moins souvent reçu de médicaments pour contrôler la fréquence ou le rythme cardiaque (p < 0,0001), mais ils ont plus souvent subi une cardioversion électrique (p < 0,0001) par rapport aux patients atteints de FA secondaire. Les hommes étaient plus jeunes au moment du diagnostic d’une FA inexpliquée (45 [intervalle interquartile : 34 à 59] vs 58 [intervalle interquartile : 40 à 69] ans; p < 0,001). Après un ajustement pour l’âge au moment du diagnostic, il n’y avait pas de différence entre les sexes quant au paramètre d’évaluation principal. La survie sans événement chez les patients jeunes ayant présenté une FA inexpliquée (âge ≤ 65 ans) était de 99,4 % à un an, et de 98,3 % à trois ans. À trois ans, une ou plusieurs hospitalisations/consultations à l’urgence pour des raisons non cardiovasculaires et pour une FA sont survenues chez 56,6 % et 23,8 % de ces patients, respectivement.
Conclusions: En utilisant une définition contemporaine stricte de la FA inexpliquée, cette étude montre que cette affection est rare, majoritairement masculine, et qu’elle est associée à une excellente survie sans événement. Cependant, le taux élevé d’utilisation de soins actifs dans les hôpitaux après le diagnostic est préoccupant.
© 2021 The Authors.
Figures


References
-
- Fox C.S., Parise H., D'Agostino R.B., Sr., et al. Parental atrial fibrillation as a risk factor for atrial fibrillation in offspring. JAMA. 2004;291:2851–2855. - PubMed
-
- Fumagalli S., Said S.A.M., Laroche C., et al. Age-related differences in presentation, treatment, and outcome of patients with atrial fibrillation in Europe: The EORP-AF General Pilot Registry (EURObservational Research Programme-Atrial Fibrillation) JACC Clin Electrophysiol. 2015;1:326–334. - PubMed
-
- Brand F.N., Abbott R.D., Kannel W.B., Wolf P.A. Characteristics and prognosis of lone atrial fibrillation: 30-year follow-up in the Framingham Study. JAMA. 1985;254:3449–3453. - PubMed
-
- Jahangir A., Lee V., Friedman P.A., et al. Long-term progression and outcomes with aging in patients with lone atrial fibrillation: a 30-year follow-up study. Circulation. 2007;115:3050–3056. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
