

Association of Ischemic Stroke Incidence, Severity, and Recurrence With Dementia in the Atherosclerosis Risk in Communities Cohort Study
- PMID: 35072712
- PMCID: PMC8787684
- DOI: 10.1001/jamaneurol.2021.5080
Association of Ischemic Stroke Incidence, Severity, and Recurrence With Dementia in the Atherosclerosis Risk in Communities Cohort Study
Abstract
Importance: Ischemic stroke is associated with increased risk of dementia, but the association of stroke severity and recurrence with risk of impaired cognition is not well known.
Objective: To examine the risk of dementia after incident ischemic stroke and assess how it differed by stroke severity and recurrence.
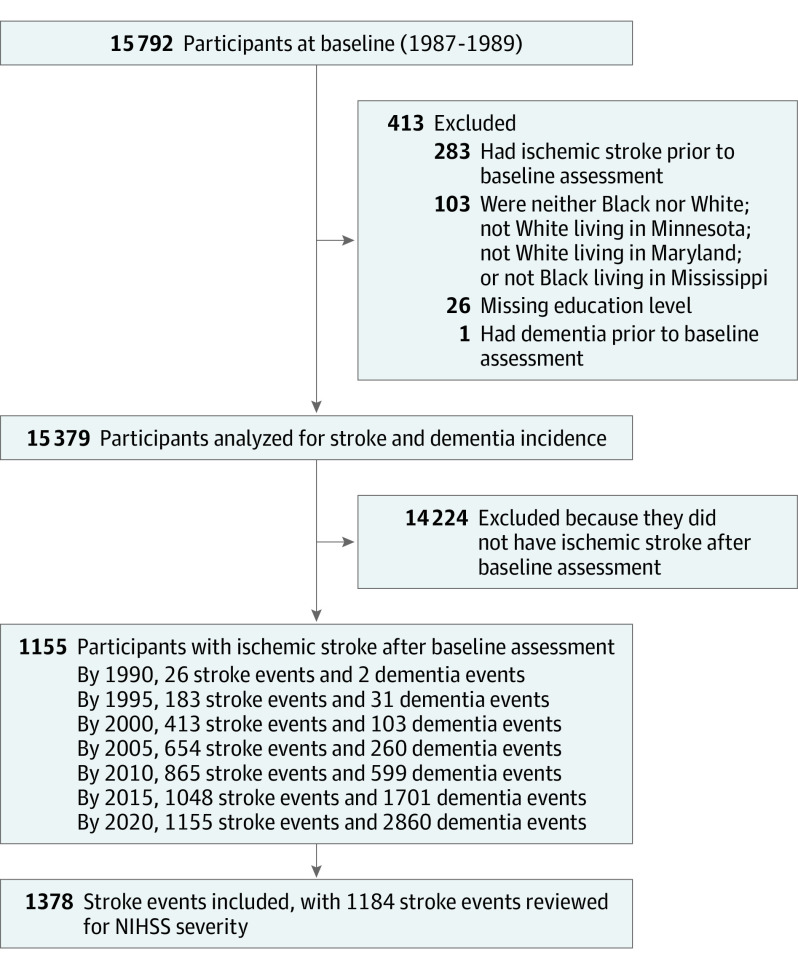
Design, setting, and participants: The Atherosclerosis Risk in Communities (ARIC) study is an ongoing prospective cohort of 15 792 community-dwelling individuals from 4 US states (Mississippi, Maryland, Minnesota, and North Carolina). Among them, 15 379 participants free of stroke and dementia at baseline (1987 to 1989) were monitored through 2019. Data were analyzed from April to October 2021. Associations between dementia and time-varying ischemic stroke incidence, frequency, and severity were studied across an average of 4.4 visits over a median follow-up of 25.5 years with Cox proportional hazards models adjusted for sociodemographic characteristics, apolipoprotein E, and vascular risk factors.
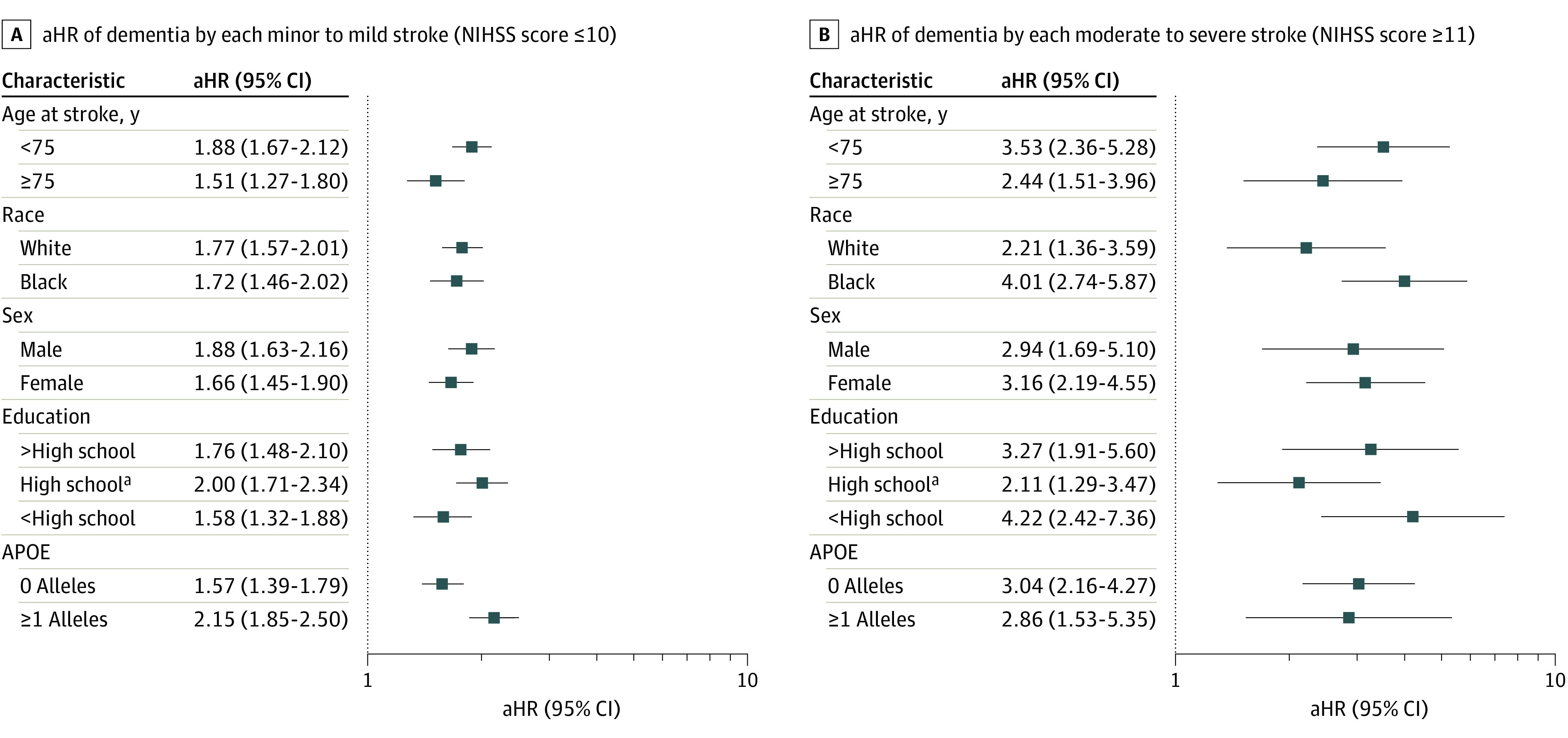
Exposures: Incident and recurrent ischemic strokes were classified by expert review of hospital records, with severity defined by the National Institutes of Health Stroke Scale (NIHSS; minor, ≤5; mild, 6-10; moderate, 11-15; and severe, ≥16).
Main outcomes and measures: Dementia cases adjudicated through expert review of in-person evaluations, informant interviews, telephone assessments, hospitalization codes, and death certificates. In participants with stroke, dementia events in the first year after stroke were not counted.
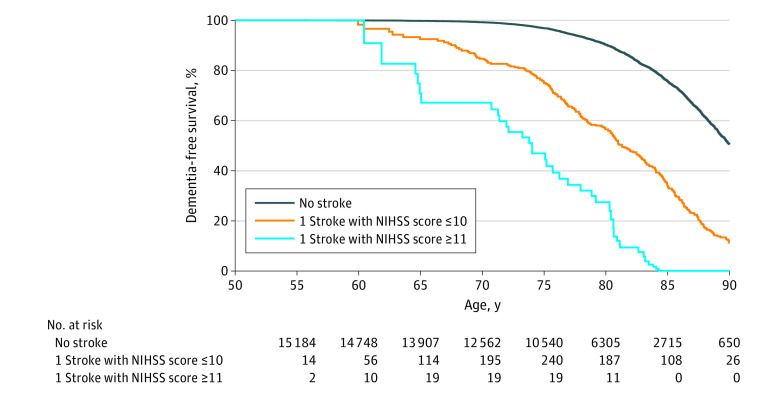
Results: At baseline, the mean (SD) age of participants was 54.1 (5.8) years, and 8485 of 15 379 participants (55.2%) were women. A total of 4110 participants (26.7%) were Black and 11 269 (73.3%) were White. A total of 1378 ischemic strokes (1155 incident) and 2860 dementia cases were diagnosed 1 year or more after incident stroke in participants with stroke, or at any point after baseline in participants without stroke, were identified through December 31, 2019. NIHSS scores were available for 1184 of 1378 ischemic strokes (85.9%). Risk of dementia increased with both the number and severity of strokes. Compared with no stroke, risk of dementia by adjusted hazard ratio was 1.76 (95% CI, 1.49-2.00) for 1 minor to mild stroke, 3.47 (95% CI, 2.23-5.40) for 1 moderate to severe stroke, 3.48 (95% CI, 2.54-4.76) for 2 or more minor to mild strokes, and 6.68 (95% CI, 3.77-11.83) for 2 or more moderate to severe strokes.
Conclusions and relevance: In this study, risk of dementia significantly increased after ischemic stroke, independent of vascular risk factors. Results suggest a dose-response association of stroke severity and recurrence with risk of dementia.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
- U01 HL096812/HL/NHLBI NIH HHS/United States
- K24 AG052573/AG/NIA NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- K23 NS112459/NS/NINDS NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
