

Treating refractory corneal hydrops in a male patient with vernal keratoconjunctivitis and mental retardation: a case report
- PMID: 35073856
- PMCID: PMC8785578
- DOI: 10.1186/s12886-021-02241-6
Treating refractory corneal hydrops in a male patient with vernal keratoconjunctivitis and mental retardation: a case report
Abstract
Background: Keratoconus is the most common noninflammatory bilateral corneal ectasia. Vernal keratoconjunctivitis (VKC) and eye rubbing may be associated with keratoconus in children and young adults. Timely management of advanced keratoconus is important to improve visual quality. In addition, it is challenging to carry out VKC treatment with an intent to avoid the occurrence of punctate epithelial keratitis, ulceration, or corneal neovascularization on corneal grafts.
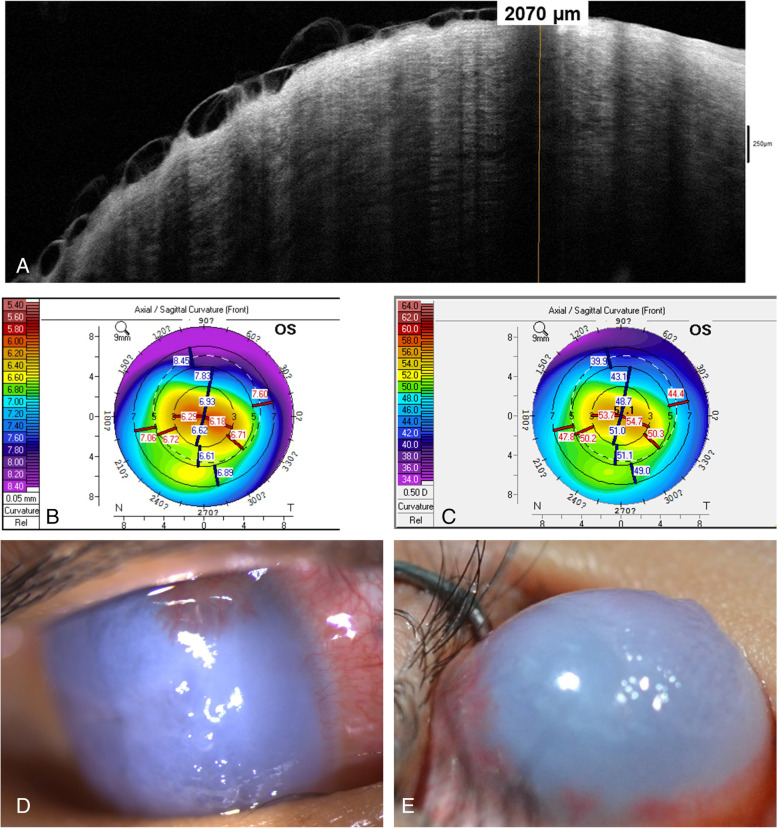
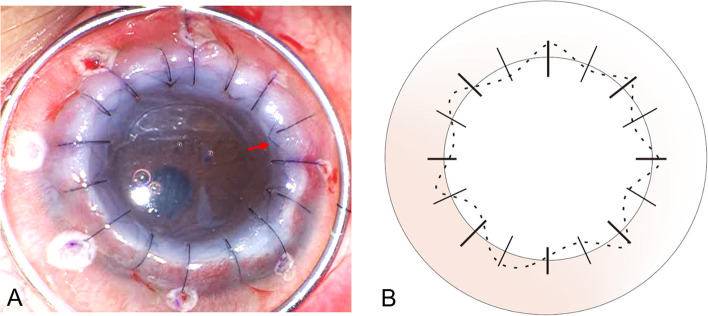
Case presentation: We report the case of an 18-year-old male patient with a long-term history of mental retardation due to megalencephaly presenting with acute onset of corneal hydrops with prominent bulging and refractory steroid-induced glaucoma of the right eye. The topography of the right eye was unavailable due to advanced ectasia, and that of the left eye revealed central steepening with inferior-superior dioptric asymmetry. According to the clinical findings, the patient was diagnosed with keratoconus. Because of progressive corneal opacity and neovascularization, the patient underwent penetrating keratoplasty (PK) with combination of interrupted and intrastromal running suturing after receiving a preoperative subconjunctival injection of bevacizumab in his right eye, followed by lower eyelid correction. After surgery, the patient was treated with 0.1% tacrolimus dermatological ointment, 0.1% cyclosporine eye drops, artificial tears, and 0.5% loteprednol for keratoplasty and VKC. Repeated education on avoiding eye rubbing was offered to the patient. Two years after PK treatment, his best-corrected visual acuity of the right eye successfully improved from hand motion at 10 cm preoperatively to 6/20 postoperatively.
Conclusions: Large-diameter PK with intrastromal suturing technique for advanced keratoconus could achieve better visual outcomes and avoid suture-related complications. In addition, tacrolimus dermatological ointment rather than tacrolimus topical eye drops or ointment showed satisfactory efficacy when combined with topical cyclosporine and steroid that no significant VKC reactivation were noted after PK.
Keywords: Case report; Corneal hydrops; Intrastromal suturing; Keratoconus; Penetrating keratoplasty; Tacrolimus; Vernal keratoconjunctivitis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Corneal hydrops associated with vernal conjunctivitis as a presenting sign of keratoconus in children.Ophthalmology. 1995 Dec;102(12):2046-9. doi: 10.1016/s0161-6420(95)30755-5. Ophthalmology. 1995. PMID: 9098316
-
Corneal ectasia in vernal keratoconjunctivitis.Ophthalmology. 1989 Nov;96(11):1615-23. doi: 10.1016/s0161-6420(89)32677-7. Ophthalmology. 1989. PMID: 2616147
-
Safety and Efficacy of Corneal Cross-linking in Pediatric Patients with Keratoconus and Vernal Keratoconjunctivitis.Middle East Afr J Ophthalmol. 2019 Aug 26;26(2):95-100. doi: 10.4103/meajo.MEAJO_240_18. eCollection 2019 Apr-Jun. Middle East Afr J Ophthalmol. 2019. PMID: 31543667 Free PMC article.
-
Management of corneal complications in vernal keratoconjunctivitis: A review.Ocul Surf. 2021 Jan;19:282-289. doi: 10.1016/j.jtos.2020.10.005. Epub 2020 Oct 24. Ocul Surf. 2021. PMID: 33148465 Review.
-
Vernal keratoconjunctivitis and keratoconus.Curr Opin Allergy Clin Immunol. 2021 Oct 1;21(5):507-514. doi: 10.1097/ACI.0000000000000765. Curr Opin Allergy Clin Immunol. 2021. PMID: 34269743 Review.
Cited by
-
Vernal Keratoconjunctivitis: A Systematic Review.Clin Rev Allergy Immunol. 2023 Aug;65(2):277-329. doi: 10.1007/s12016-023-08970-4. Epub 2023 Sep 2. Clin Rev Allergy Immunol. 2023. PMID: 37658939 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
