

Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): a phase 4, non-inferiority, single blind, randomised study
- PMID: 35074136
- PMCID: PMC8782575
- DOI: 10.1016/S0140-6736(22)00094-0
Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): a phase 4, non-inferiority, single blind, randomised study
Abstract
Introduction: The inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac, Sinovac) has been widely used in a two-dose schedule. We assessed whether a third dose of the homologous or a different vaccine could boost immune responses.
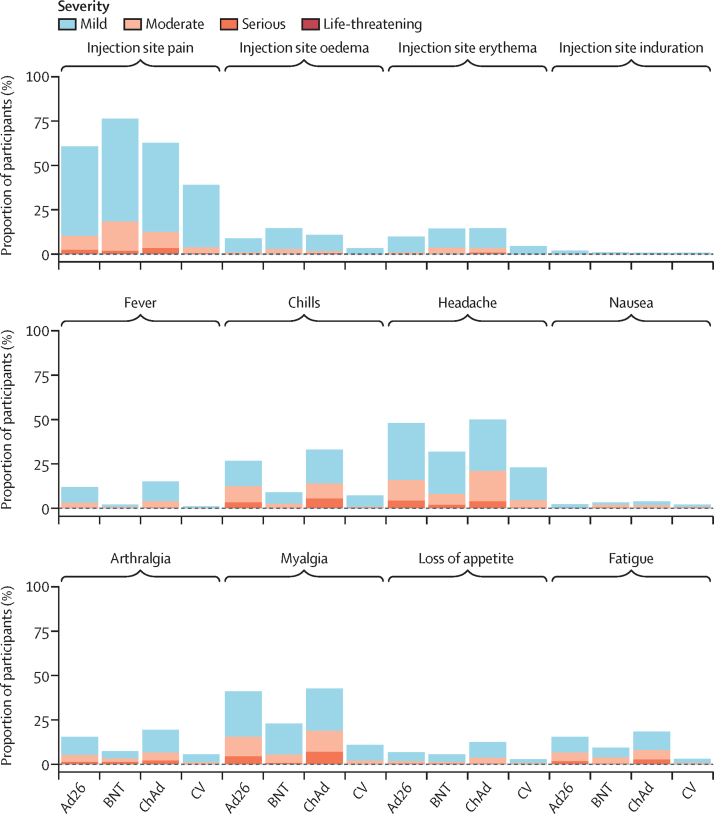
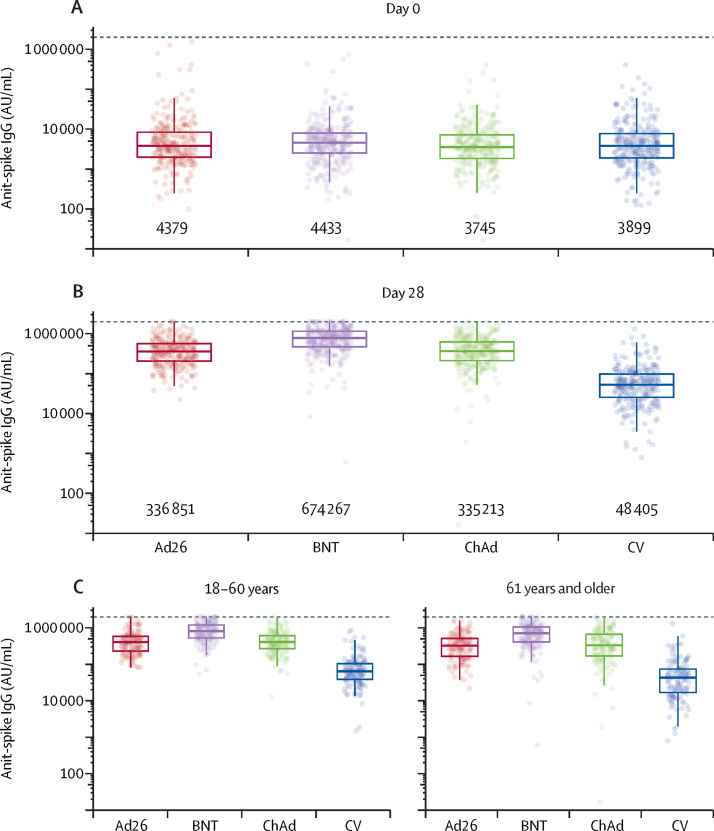
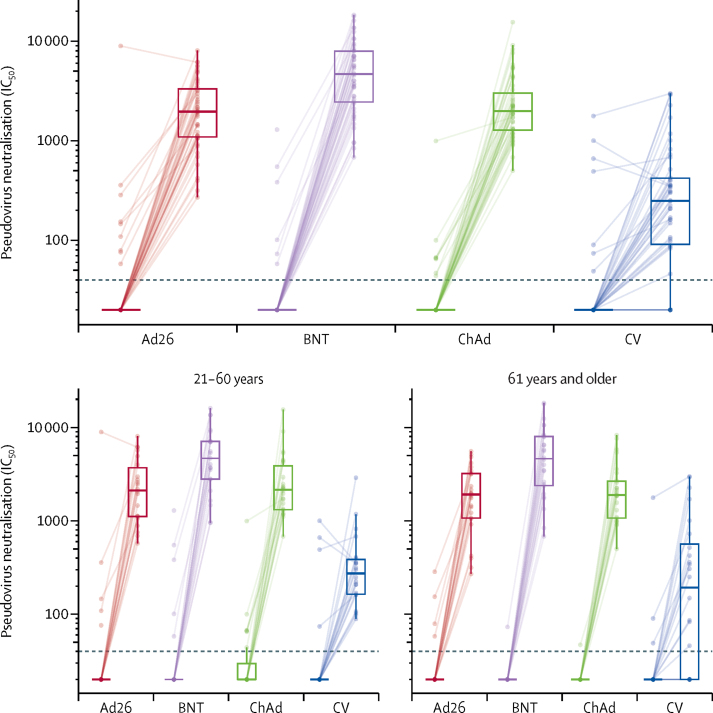
Methods: RHH-001 is a phase 4, participant masked, two centre, safety and immunogenicity study of Brazilian adults (18 years and older) in São Paulo or Salvador who had received two doses of CoronaVac 6 months previously. The third heterologous dose was of either a recombinant adenoviral vectored vaccine (Ad26.COV2-S, Janssen), an mRNA vaccine (BNT162b2, Pfizer-BioNTech), or a recombinant adenoviral-vectored ChAdOx1 nCoV-19 vaccine (AZD1222, AstraZeneca), compared with a third homologous dose of CoronaVac. Participants were randomly assigned (5:6:5:5) by a RedCAP computer randomisation system stratified by site, age group (18-60 years or 61 years and over), and day of randomisation, with a block size of 42. The primary outcome was non-inferiority of anti-spike IgG antibodies 28 days after the booster dose in the heterologous boost groups compared with homologous regimen, using a non-inferiority margin for the geometric mean ratio (heterologous vs homologous) of 0·67. Secondary outcomes included neutralising antibody titres at day 28, local and systemic reactogenicity profiles, adverse events, and serious adverse events. This study was registered with Registro Brasileiro de Ensaios Clínicos, number RBR-9nn3scw.
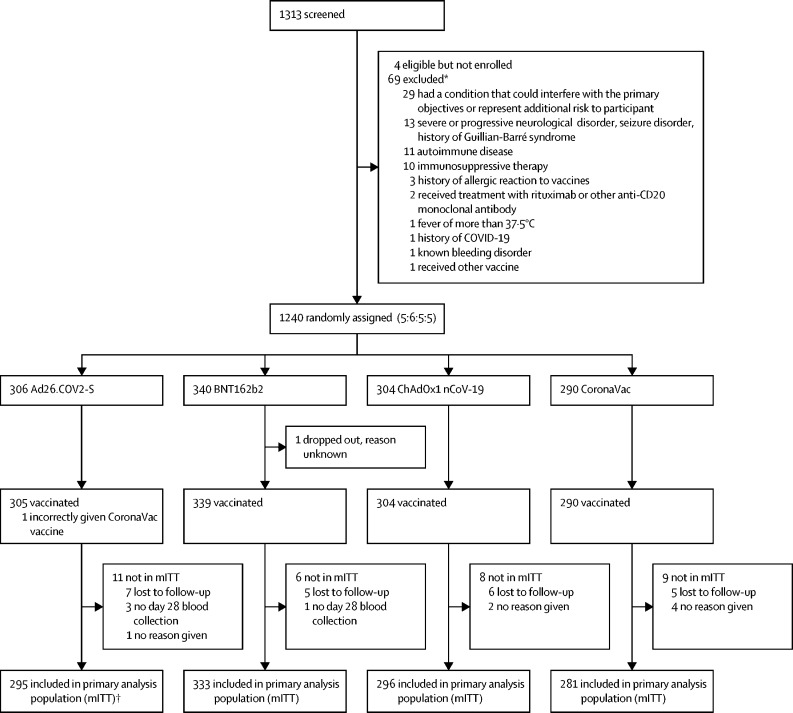
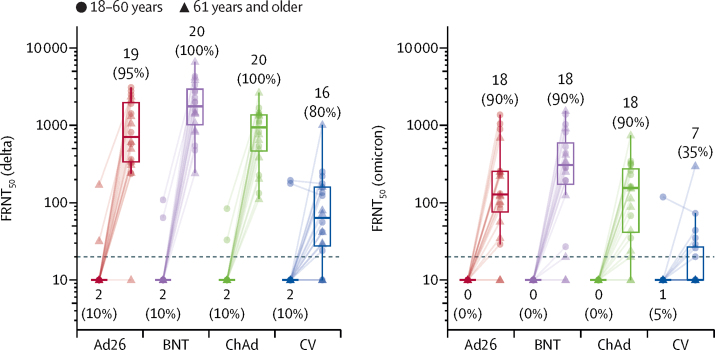
Findings: Between Aug 16, and Sept 1, 2021, 1240 participants were randomly assigned to one of the four groups, of whom 1239 were vaccinated and 1205 were eligible for inclusion in the primary analysis. Antibody concentrations were low before administration of a booster dose with detectable neutralising antibodies of 20·4% (95% CI 12·8-30·1) in adults aged 18-60 years and 8·9% (4·2-16·2) in adults 61 years or older. From baseline to day 28 after the booster vaccine, all groups had a substantial rise in IgG antibody concentrations: the geometric fold-rise was 77 (95% CI 67-88) for Ad26.COV2-S, 152 (134-173) for BNT162b2, 90 (77-104) for ChAdOx1 nCoV-19, and 12 (11-14) for CoronaVac. All heterologous regimens had anti-spike IgG responses at day 28 that were superior to homologous booster responses: geometric mean ratios (heterologous vs homologous) were 6·7 (95% CI 5·8-7·7) for Ad26.COV2-S, 13·4 (11·6-15·3) for BNT162b2, and 7·0 (6·1-8·1) for ChAdOx1 nCoV-19. All heterologous boost regimens induced high concentrations of pseudovirus neutralising antibodies. At day 28, all groups except for the homologous boost in the older adults reached 100% seropositivity: geometric mean ratios (heterologous vs homologous) were 8·7 (95% CI 5·9-12·9) for Ad26.COV2-S vaccine, 21·5 (14·5-31·9) for BNT162b2, and 10·6 (7·2-15·6) for ChAdOx1 nCoV-19. Live virus neutralising antibodies were also boosted against delta (B.1.617.2) and omicron variants (B.1.1.529). There were five serious adverse events. Three of which were considered possibly related to the vaccine received: one in the BNT162b2 group and two in the Ad26.COV2-S group. All participants recovered and were discharged home.
Interpretation: Antibody concentrations were low at 6 months after previous immunisation with two doses of CoronaVac. However, all four vaccines administered as a third dose induced a significant increase in binding and neutralising antibodies, which could improve protection against infection. Heterologous boosting resulted in more robust immune responses than homologous boosting and might enhance protection.
Funding: Ministry of Health, Brazil.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests AJP is chair of the UK Department of Health and Social Care's Joint Committee on Vaccination and Immunisation, but does not participate in policy advice on coronavirus vaccines, and is a member of the WHO Strategic Advisory Group of Experts. AJP is an National Institute for Health Research Senior Investigator. TL is named as an inventor on a patent application covering ChAdOx1 nCoV-19. Oxford University has entered into a partnership with AstraZeneca for further development of ChAdOx1 nCoV-19. All other authors declare no competing interests.
Figures
Comment in
-
Boosting immunity after CoronaVac.Lancet. 2022 Feb 5;399(10324):496-497. doi: 10.1016/S0140-6736(22)00095-2. Epub 2022 Jan 21. Lancet. 2022. PMID: 35074137 Free PMC article. No abstract available.
References
-
- Palacios R, Batista AP, Albuquerque CSN, et al. Efficacy and safety of a COVID-19 inactivated vaccine in healthcare professionals in Brazil: the PROFISCOV study. SSRN. 2021 doi: 10.2139/ssrn.3822780. published online April 14. (preprint). - DOI
-
- Li M, Yang J, Wang L, et al. A booster dose is immunogenic and will be needed for older adults who have completed two doses vaccination with CoronaVac: a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. medRxiv. 2021 doi: 10.1101/2021.08.03.21261544. published online Aug 8. (preprint). - DOI
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
