

Effective Anti-SARS-CoV-2 Immune Response in Patients With Clonal Mast Cell Disorders
- PMID: 35074600
- PMCID: PMC8780123
- DOI: 10.1016/j.jaip.2021.12.038
Effective Anti-SARS-CoV-2 Immune Response in Patients With Clonal Mast Cell Disorders
Abstract
Background: Mast cells are key players in innate immunity and the TH2 adaptive immune response. The latter counterbalances the TH1 response, which is critical for antiviral immunity. Clonal mast cell activation disorders (cMCADs, such as mastocytosis and clonal mast cell activation syndrome) are characterized by abnormal mast cell accumulation and/or activation. No data on the antiviral immune response in patients with MCADs have been published.
Objective: To study a comprehensive range of outcomes in patients with cMCAD with PCR- or serologically confirmed coronavirus disease 2019 and to characterize the specific anti-severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) immune response in this setting.
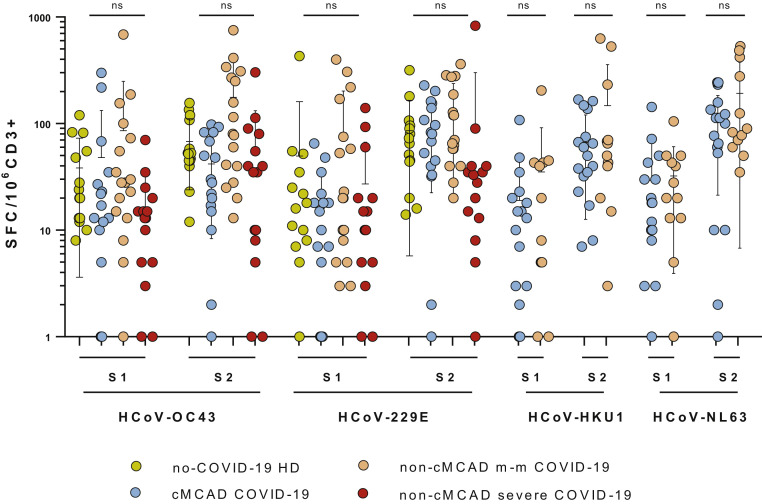
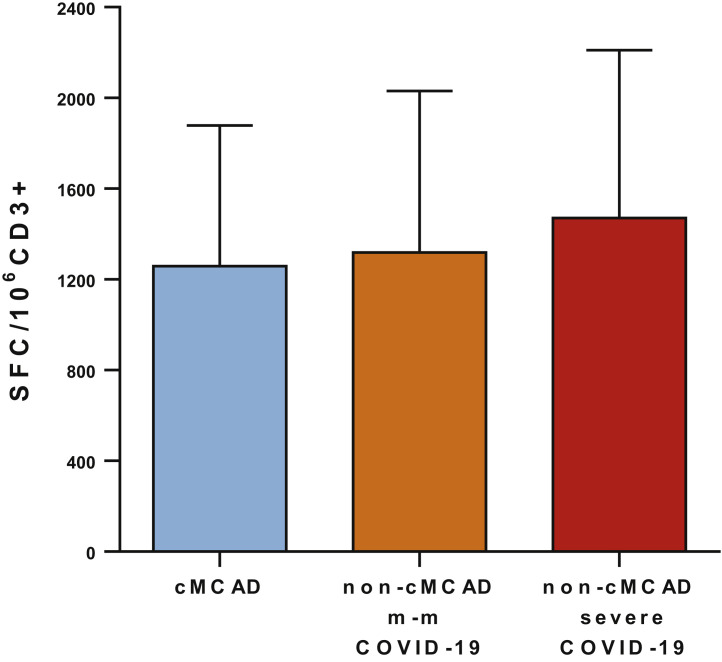
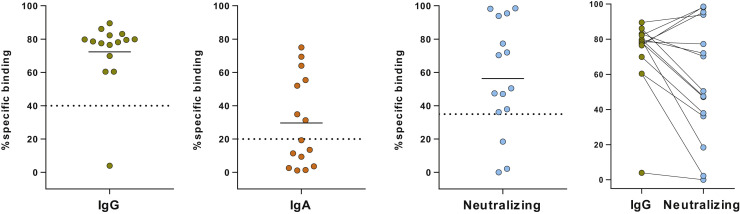
Methods: Clinical follow-up and outcome data were collected prospectively over a 12-month period by members of the French Centre de Référence des Mastocytoses rare disease network. Anti-SARS-CoV-2-specific T-cell activity was measured with an ELISA, and humoral responses were evaluated by assaying circulating levels of specific IgG, IgA, and neutralizing antibodies.
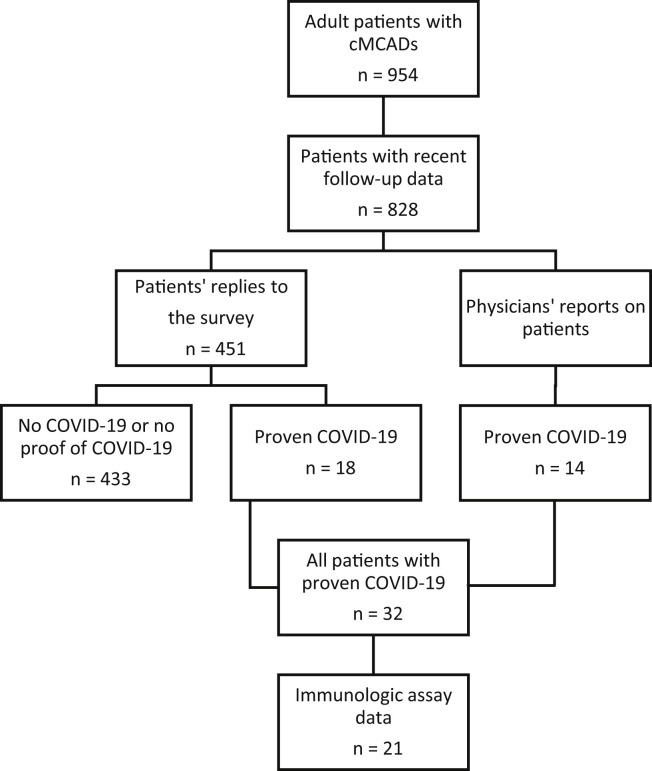
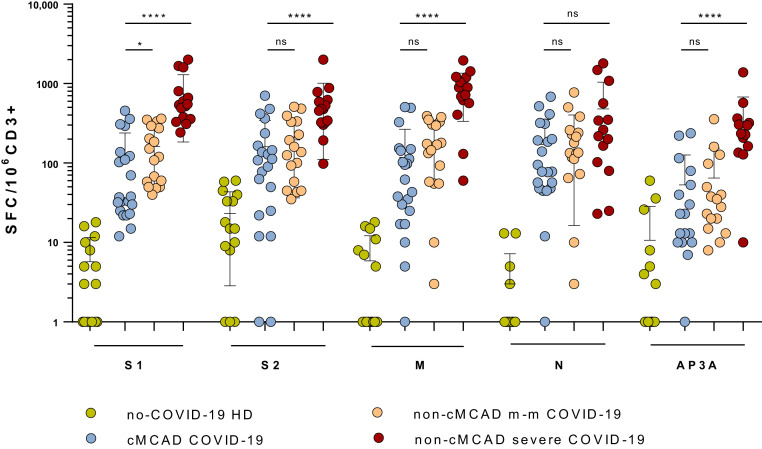
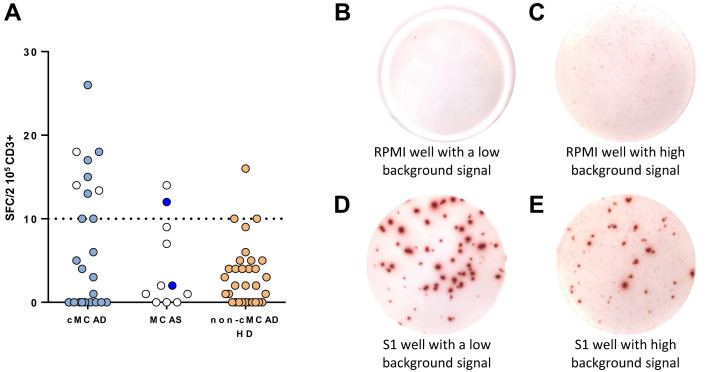
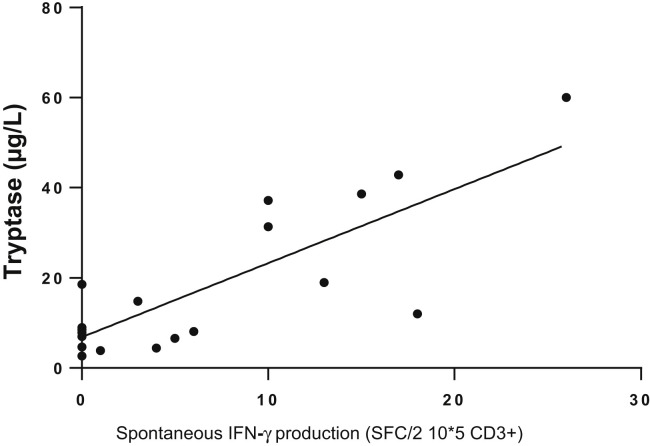
Results: Overall, 32 patients with cMCAD were evaluated. None required noninvasive or mechanical ventilation. Two patients were admitted to hospital for oxygen and steroid therapy. The SARS-CoV-2-specific immune response was characterized in 21 of the 32 patients. Most had high counts of circulating SARS-CoV-2-specific, IFN-γ-producing T cells and high titers of neutralizing antispike IgGs. The patients frequently showed spontaneous T-cell IFN-γ production in the absence of stimulation; this production was correlated with basal circulating tryptase levels (a marker of the mast cell burden).
Conclusions: Patients with cMCADs might not be at risk of severe coronavirus disease 2019, perhaps due to their spontaneous production of IFN-γ.
Keywords: B cells; COVID-19; Clonal mast cell activation syndrome; Mast cell activation disorders; Mast cells; Mastocytosis; SARS-CoV-2; T cells.
Copyright © 2022. Published by Elsevier Inc.
Figures
References
-
- Lim K., Tefferi A., Lasho T.L., Finke C., Patnaik M., Butterfield J.H., et al. Systemic mastocytosis in 342 consecutive adults: survival studies and prognostic factors. Blood. 2009;113:5727–5736. - PubMed
-
- Gotlib J., Pardanani A., Akin C., Reiter A., George T., Hermine O., et al. International Working Group-Myeloproliferative Neoplasms Research and Treatment (IWG-MRT) & European Competence Network on Mastocytosis (ECNM) consensus response criteria in advanced systemic mastocytosis. Blood. 2013;121:2393–2401. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
