

Lymphedema and Obesity
- PMID: 35074795
- PMCID: PMC9159261
- DOI: 10.1101/cshperspect.a041176
Lymphedema and Obesity
Abstract
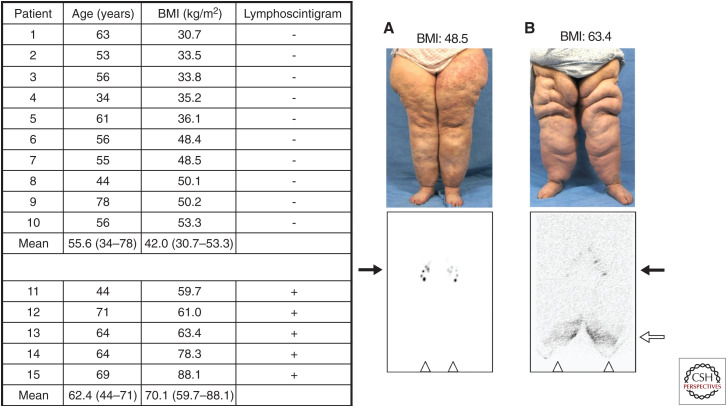
Lymphedema results from inadequate lymphatic function. Extreme obesity can cause lower extremity lymphedema, termed "obesity-induced lymphedema (OIL)." OIL is a form of secondary lymphedema that may occur once an individual's body mass index (BMI) exceeds 40. The risk of lymphatic dysfunction increases with elevated BMI and is almost universal once BMI exceeds 60. Obesity has a negative impact on lymphatic density in subcutaneous tissue, lymphatic endothelial cell proliferation, lymphatic leakiness, collecting-vessel pumping capacity, and clearance of macromolecules. Lymphatic fluid unable to be taken up by lymphatic vessels results in increased subcutaneous adipose deposition, fibrosis, and worsening obesity. Individuals with OIL are in an unfavorable cycle of weight gain and lymphatic injury. The fundamental treatment for OIL is weight loss.
Copyright © 2022 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical