

doi: 10.1002/ctm2.648.
COVID-19 bimodal clinical and pathological phenotypes
Affiliations
- PMID: 35075808
- PMCID: PMC8787021
- DOI: 10.1002/ctm2.648
Item in Clipboard
COVID-19 bimodal clinical and pathological phenotypes
Clin Transl Med.
2022 Jan.
No abstract available
Conflict of interest statement
The authors declare no conflict of interest.
Figures
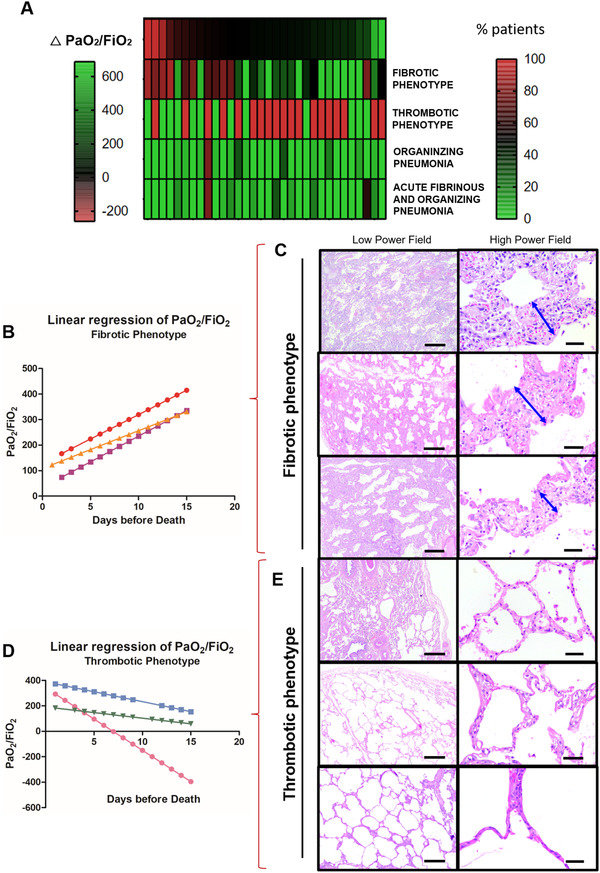
COVID‐19 bimodal clinical and pathological phenotypes. After a multidisciplinary discussion and data integration and analysis, bimodal clinical and pathological phenotypes of COVID‐19 minimally invasive autopsies were discovered by PaO2/FiO2 linear regression and lung morphology correlation, presented as a gradient (A). The two opposite ends of lung injury were named as (1) Fibrotic phenotype (N = 5) presenting progressive decline in PaO2/FiO2 ratio (B) with significant alveolar septal thickening by fibrosis (C–double blue arrows) without thrombus formation (C); and (2) Thrombotic Phenotype (N = 10) presenting a progressive increase in PaO2/FiO2 ratio (D) with recovery of acute/sub‐acute lung injury to or near to normal parenchyma architecture and thrombus formation on vessels (E). Between both phenotypes, a population (N = 32) of non‐bimodal phenotype with different stages of acute, organizing and fibrotic lung injury (A). Scale bar indicates 500 μm in the low power field and 50 μm in high power field (C and E)
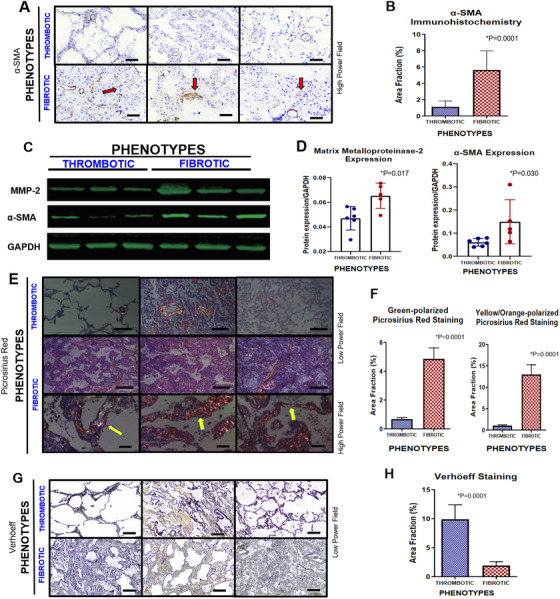
Pulmonary morphological panels of COVID‐19 bimodal phenotypes. Cells expressing α‐SMA by immunohistochemistry were highlighted in fibrotic phenotype compared to thrombotic one (red arrows), probably induced by myofibroblastic activation and neovasculogenesis (A). The α‐SMA expression is confirmed by morphometric analysis (B). Protein expression levels of α‐SMA and MMP‐2 were performed by Western blot (C). GAPDH was used as gene expression control (C–last line). Their quantification was also increased in fibrotic phenotype compared to thrombotic one, confirming the disbalance of production/degradation of extracellular matrix (D). Additionally, extracellular matrix deposition was confirmed by alveolar septal thickening in fibrotic phenotype seen by polarized birefringence of Picrosirius red staining (E–yellow arrow). Morphometric analysis of green and yellow orange polarized collagen fibers by Picrosirius red staining was significantly higher in fibrotic phenotype than thrombotic one (F). Inversely, lung elastic fibers related to elastic tissue capacity were rarefied in fibrotic phenotype by Verhöeff staining compared to thrombotic one (G). This finding was confirmed by morphometric analysis (H). Scale bar indicates 50 μm in high power field (A and E) and 200 μm in low power field (E and G)
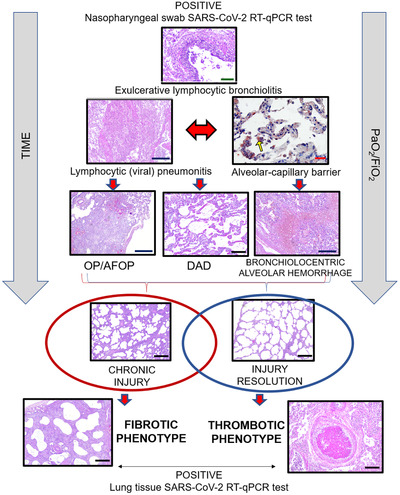
COVID‐19 lung pathophysiology. The viral infection starts in the lungs first by reaching the airways and infecting bronchial epithelial cells. Then, the pathophysiological processes in response to the viral attack cause an exulcerating lymphocytic bronchiolitis, followed by lymphocytic (viral) pneumonitis. Consequently, the second wave of infection overspreads through the lung parenchyma, inducing cellular pneumonitis, which injures the alveolo‐capillar barriers near distal airways, highlighted by immunohistochemistry with anti‐SARS‐CoV‐2 (yellow arrow). Then, fibroplastic balls (organizing pneumonia–OP) and fibrin balls (acute fibrinous and organizing pneumonia–AFOP), diffuse alveolar damaged (DAD) and bronchiolocentric alveolar hemorrhage may occur in the injured lung tissue. Over the time of viral infection and mechanical ventilation, two different repair processes can occur depending on the resolution or progression of the injury, coinciding with the bimodal clinic‐pathological phenotype: (1) Chronic injury with fibrotic phenotype; or (2) Gradual injury resolution with thrombotic phenotype. Scale bars indicate: 500 μm (blue), 200 μm (black), 100 μm (green) and 50 μm (red)
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical