

Clinical applications of cardiac computed tomography: a consensus paper of the European Association of Cardiovascular Imaging-part I
- PMID: 35076061
- PMCID: PMC8863074
- DOI: 10.1093/ehjci/jeab293
Clinical applications of cardiac computed tomography: a consensus paper of the European Association of Cardiovascular Imaging-part I
Erratum in
-
Erratum to: Clinical applications of cardiac computed tomography: a consensus paper of the European Association of Cardiovascular Imaging-part I.Eur Heart J Cardiovasc Imaging. 2022 Jun 1;23(6):e274. doi: 10.1093/ehjci/jeac047. Eur Heart J Cardiovasc Imaging. 2022. PMID: 35403685 Free PMC article. No abstract available.
Abstract
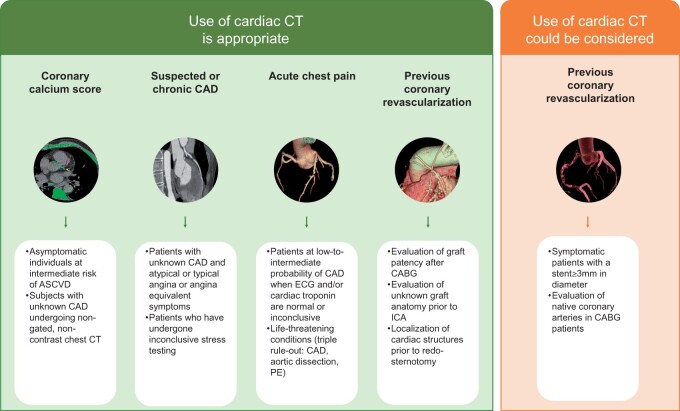
Cardiac computed tomography (CT) was introduced in the late 1990's. Since then, an increasing body of evidence on its clinical applications has rapidly emerged. From an initial emphasis on its technical efficiency and diagnostic accuracy, research around cardiac CT has now evolved towards outcomes-based studies that provide information on prognosis, safety, and cost. Thanks to the strong and compelling data generated by large, randomized control trials, the scientific societies have endorsed cardiac CT as pivotal diagnostic test for the management of appropriately selected patients with acute and chronic coronary syndrome. This consensus document endorsed by the European Association of Cardiovascular Imaging is divided into two parts and aims to provide a summary of the current evidence and to give updated indications on the appropriate use of cardiac CT in different clinical scenarios. This first part focuses on the most established applications of cardiac CT from primary prevention in asymptomatic patients, to the evaluation of patients with chronic coronary syndrome, acute chest pain, and previous coronary revascularization.
Keywords: acute chest pain; chronic coronary syndrome; coronary artery bypass graft; coronary calcium; coronary computed tomography angiography; coronary stent.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2022. For permissions, please email: journals.permissions@oup.com.
Figures

References
-
- Lackner K, Thurn P. Computed tomography of the heart: ECG-gated and continuous scans. Radiology 1981;140:413–20. - PubMed
-
- Lipton MJ, Higgins CB, Boyd DP. Computed tomography of the heart: evaluation of anatomy and function. J Am Coll Cardiol 1985;5:55S–69S. - PubMed
-
- Achenbach S, Ulzheimer S, Baum U, Kachelriess M, Ropers D, Giesler T et al. Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation 2000;102:2823–8. - PubMed
-
- Nieman K, Oudkerk M, Rensing BJ, van Ooijen P, Munne A, van Geuns RJ et al. Coronary angiography with multi-slice computed tomography. Lancet 2001;357:599–603. - PubMed
-
- Marano R, De Cobelli F, Floriani I, Becker C, Herzog C, Centonze M et al.; NIMISCAD Study Group. Italian multicenter, prospective study to evaluate the negative predictive value of 16- and 64-slice MDCT imaging in patients scheduled for coronary angiography (NIMISCAD-Non Invasive Multicenter Italian Study for Coronary Artery Disease). Eur Radiol 2009;19:1114–23. - PubMed
