

Diagnosis, consultation, treatment, and impact of migraine in the US: Results of the OVERCOME (US) study
- PMID: 35076091
- PMCID: PMC9305407
- DOI: 10.1111/head.14259
Diagnosis, consultation, treatment, and impact of migraine in the US: Results of the OVERCOME (US) study
Abstract
Objective: The ObserVational survey of the Epidemiology, tReatment and Care of MigrainE (OVERCOME; United States) study is a multicohort, longitudinal web survey that assesses symptomatology, consulting, diagnosis, treatment, and impact of migraine in the United States.
Background: Regularly updating population-based views of migraine in the United States provides a method for assessing the quality of ongoing migraine care and identifying unmet needs.
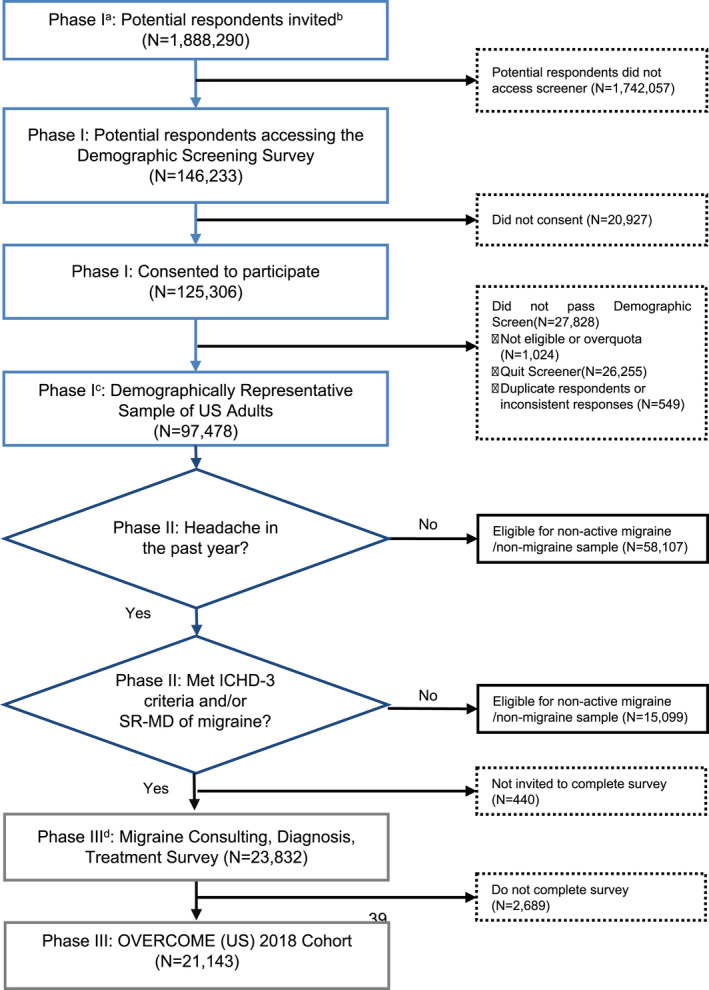
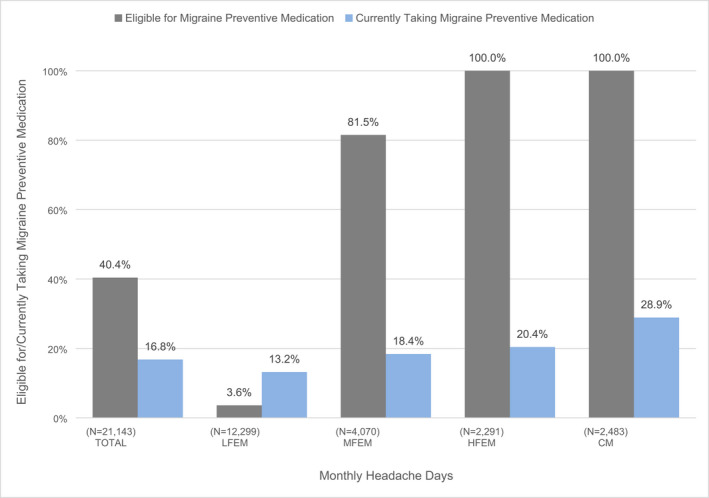
Methods: The OVERCOME (US) 2018 migraine cohort involved: (I) creating a demographically representative sample of US adults using quota sampling (n = 97,478), (II) identifying people with active migraine in the past year via a validated migraine diagnostic questionnaire and/or self-reported medical diagnosis of migraine (n = 24,272), and (III) assessing consultation, diagnosis, and treatment of migraine (n = 21,143). The current manuscript evaluated whether those with low frequency episodic migraine (LFEM; 0-3 monthly headache days) differed from other categories on outcomes of interest.
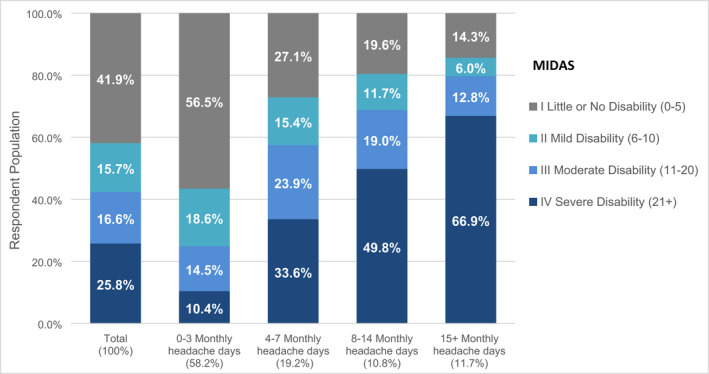
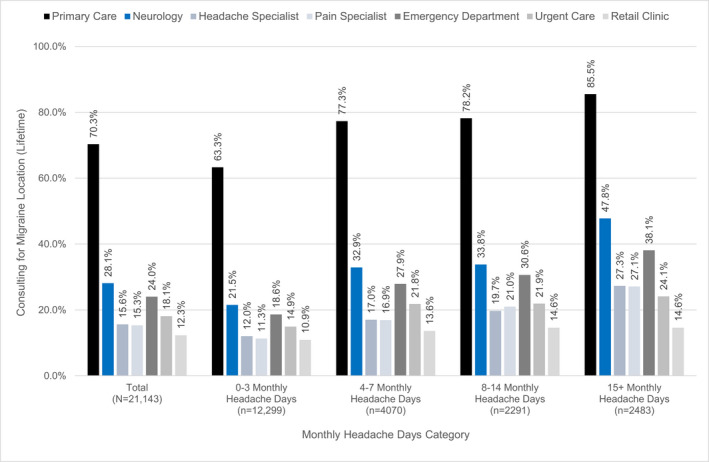
Results: Among the migraine cohort (n = 21,143), 19,888 (94.1%) met our International Classification of Headache Disorders, 3rd edition-based case definition of migraine and 12,905 (61.0%) self-reported a medical diagnosis of migraine. Respondents' mean (SD) age was 42.2 (15.0) years; 15,697 (74.2%) were women. Having at least moderate disability was common (n = 8965; 42.4%) and around half (n = 10,783; 51.0%) had consulted a medical professional for migraine care in the past year. Only 4792 (22.7%) of respondents were currently using a triptan. Overall, 8539 (40.4%) were eligible for migraine preventive medication and 3555 (16.8%) were currently using migraine preventive medication. Those with LFEM differed from moderate and high frequency episodic migraine and chronic migraine on nearly all measures of consulting, diagnosis, and treatment.
Conclusion: The OVERCOME (US) 2018 cohort revealed slow but steady progress in diagnosis and preventive treatment of migraine. However, despite significant impact among the population, many with migraine have unmet needs related to consulting for migraine, migraine diagnosis, and getting potentially beneficial migraine treatment. Moreover, it demonstrated the heterogeneity and varying unmet needs within episodic migraine.
Keywords: diagnosis; episodic migraine; headache; migraine; treatment; unmet need.
© 2022 Eli Lilly and Company. Headache: The Journal of Head and Face Pain published by Wiley Periodicals LLC on behalf of American Headache Society.
Conflict of interest statement
Richard B. Lipton, MD, has received research support from the National Institutes of Health, the FDA and the National Headache Foundation. He serves as consultant, advisory board member, or has received honoraria or research support from AbbVie/Allergan, Amgen, Biohaven, Dr. Reddy’s Laboratories (Promius), electroCore, Eli Lilly, GlaxoSmithKline, Lilly, Lundbeck, Merck, Novartis, Teva, Vector, and Vedanta Research. He receives royalties from Wolff’s Headache, 8th edition (Oxford University Press, 2009), and Informa. He holds stock/options in Biohaven and CntrlM. Robert A. Nicholson, PhD, is an employee and minor stockholder of Eli Lilly and Company. Michael L. Reed, PhD, has received research support from the National Headache Foundation. He serves as consultant, advisory board member, or has received honoraria or research support from Abbvie/Allergan, Amgen, Dr. Reddy’s Laboratories (Promius), and Eli Lilly. Andre B. Araujo, PhD, reports prior employment and is a minor stockholder of Eli Lilly and Company. Dena H. Jaffe, PhD, is an employee of Kantar Health which receives support from Eli Lilly and Company. Douglas E. Faries, PhD, is an employee and minor stockholder of Eli Lilly and Company. Dawn C. Buse, PhD, has received research support from the FDA and the National Headache Foundation. She serves as consultant, advisory board member, or has received honoraria or research support from AbbVie/Allergan, Amgen, Biohaven, Dr. Reddy’s Laboratories (Promius), Eli Lilly, Lundbeck, Novartis, and Teva. Robert E. Shapiro, MD, PhD, serves as consultant, advisory board member, or has received honoraria or research support from Eli Lilly and Lundbeck. Sait Ashina, MD, serves as consultant, advisory board member, or has received honoraria or research support from AbbVie/Allergan, Amgen, Eli Lilly, Impel NeuroPharma, Novartis, Satsuma, Supernus, and Theranica. M. Janelle Cambron‐Mellott, PhD, is an employee of Kantar Health which receives support from Eli Lilly and Company. John C. Rowland, MS, is an employee of Kantar Health which receives support from Eli Lilly and Company. Eric M. Pearlman, MD, PhD, is an employee and minor stockholder of Eli Lilly and Company.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
