

Multimodal Neural and Behavioral Data Predict Response to Rehabilitation in Chronic Poststroke Aphasia
- PMID: 35078348
- PMCID: PMC9022691
- DOI: 10.1161/STROKEAHA.121.036749
Multimodal Neural and Behavioral Data Predict Response to Rehabilitation in Chronic Poststroke Aphasia
Abstract
Background: Poststroke recovery depends on multiple factors and varies greatly across individuals. Using machine learning models, this study investigated the independent and complementary prognostic role of different patient-related factors in predicting response to language rehabilitation after a stroke.
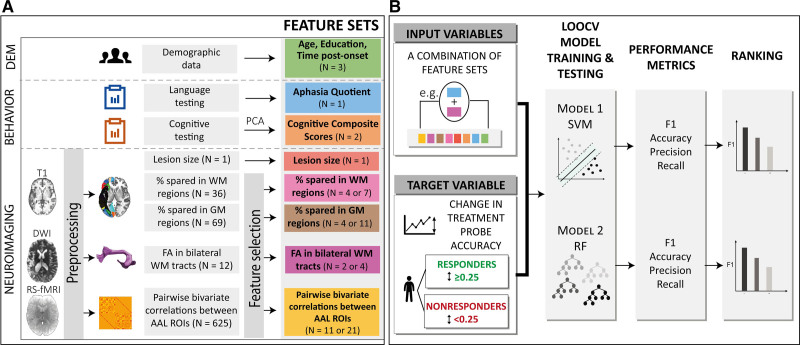
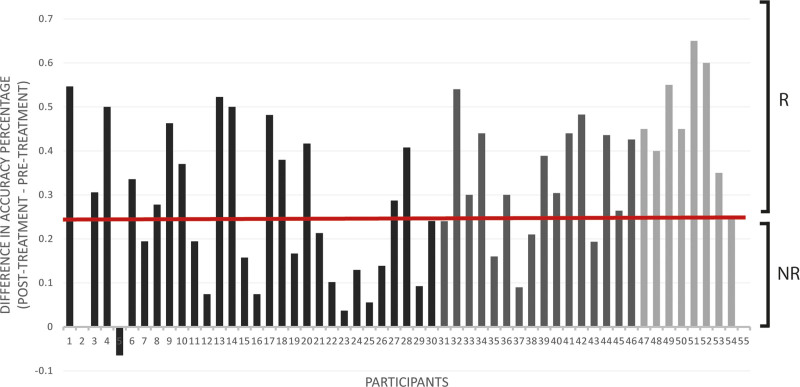
Methods: Fifty-five individuals with chronic poststroke aphasia underwent a battery of standardized assessments and structural and functional magnetic resonance imaging scans, and received 12 weeks of language treatment. Support vector machine and random forest models were constructed to predict responsiveness to treatment using pretreatment behavioral, demographic, and structural and functional neuroimaging data.
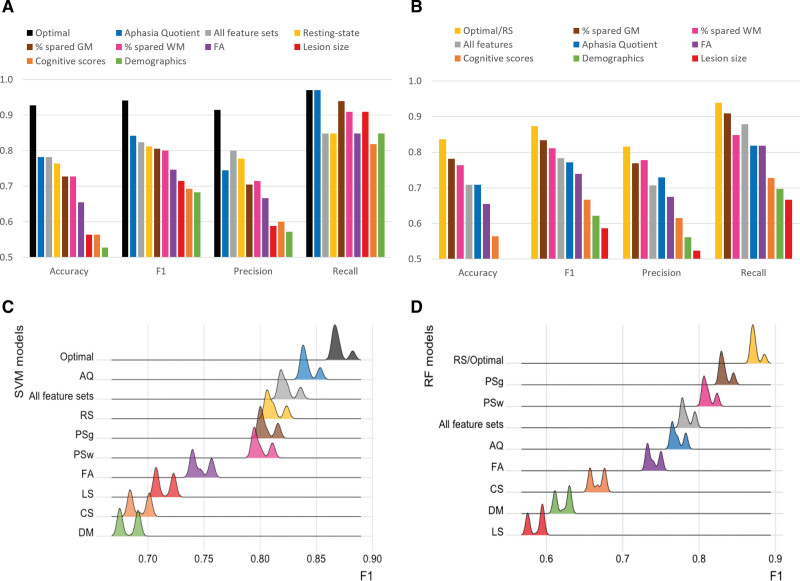
Results: The best prediction performance was achieved by a support vector machine model trained on aphasia severity, demographics, measures of anatomic integrity and resting-state functional connectivity (F1=0.94). This model resulted in a significantly superior prediction performance compared with support vector machine models trained on all feature sets (F1=0.82, P<0.001) or a single feature set (F1 range=0.68-0.84, P<0.001). Across random forest models, training on resting-state functional magnetic resonance imaging connectivity data yielded the best F1 score (F1=0.87).
Conclusions: While behavioral, multimodal neuroimaging data and demographic information carry complementary information in predicting response to rehabilitation in chronic poststroke aphasia, functional connectivity of the brain at rest after stroke is a particularly important predictor of responsiveness to treatment, both alone and combined with other patient-related factors.
Keywords: aphasia; language; machine learning; magnetic resonance imaging; neuroimaging; rehabilitation.
Figures


References
-
- Adamson J, Beswick A, Ebrahim S. Is stroke the most common cause of disability? J Stroke Cerebrovasc Dis. 2004;13:171–177. doi: 10.1016/j.jstrokecerebrovasdis.2004.06.003 - PubMed
-
- Daniel K, Wolfe CD, Busch MA, McKevitt C. What are the social consequences of stroke for working-aged adults? A systematic review. Stroke. 2009;40:e431–e440. doi: 10.1161/STROKEAHA.108.534487 - PubMed
-
- Kauhanen ML, Korpelainen JT, Hiltunen P, Määttä R, Mononen H, Brusin E, Sotaniemi KA, Myllylä VV. Aphasia, depression, and non-verbal cognitive impairment in ischaemic stroke. Cerebrovasc Dis. 2000;10:455–461. doi: 10.1159/000016107 - PubMed
-
- Watila MM, Balarabe SA. Factors predicting post-stroke aphasia recovery. J Neurol Sci. 2015;352:12–18. doi: 10.1016/j.jns.2015.03.020 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
