

Immunotherapy for glioblastoma: the promise of combination strategies
- PMID: 35078492
- PMCID: PMC8787896
- DOI: 10.1186/s13046-022-02251-2
Immunotherapy for glioblastoma: the promise of combination strategies
Abstract
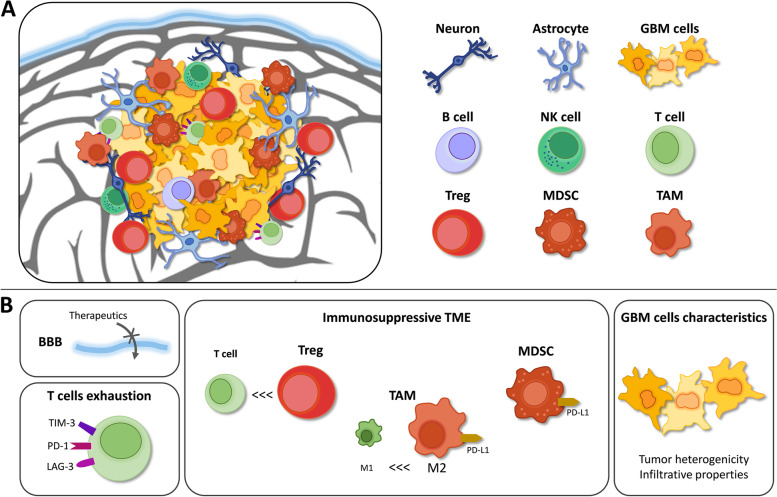
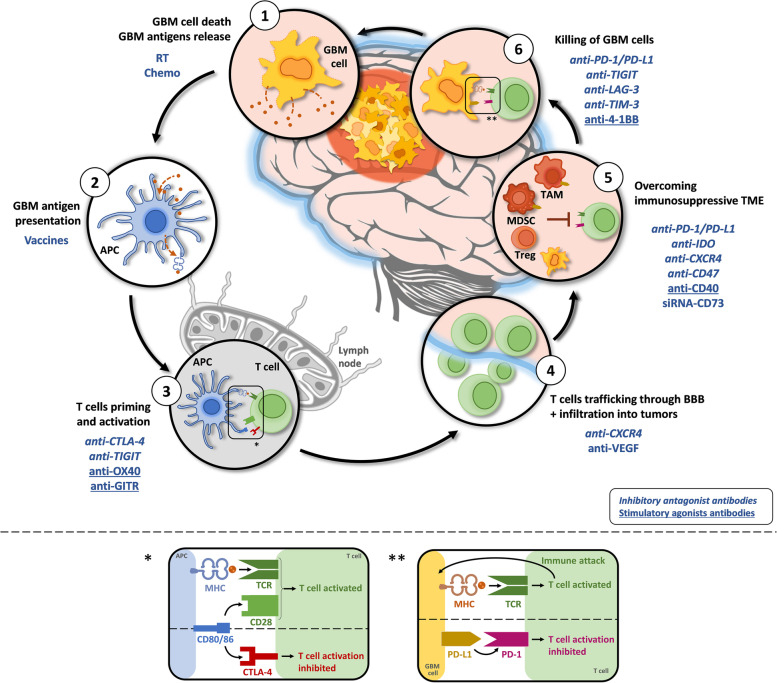
Glioblastoma (GBM) treatment has remained almost unchanged for more than 20 years. The current standard of care involves surgical resection (if possible) followed by concomitant radiotherapy and chemotherapy. In recent years, immunotherapy strategies have revolutionized the treatment of many cancers, increasing the hope for GBM therapy. However, mostly due to the high, multifactorial immunosuppression occurring in the microenvironment, the poor knowledge of the neuroimmune system and the presence of the blood-brain barrier, the efficacy of immunotherapy in GBM is still low. Recently, new strategies for GBM treatments have employed immunotherapy combinations and have provided encouraging results in both preclinical and clinical studies. The lessons learned from clinical trials highlight the importance of tackling different arms of immunity. In this review, we aim to summarize the preclinical evidence regarding combination immunotherapy in terms of immune and survival benefits for GBM management. The outcomes of recent studies assessing the combination of different classes of immunotherapeutic agents (e.g., immune checkpoint blockade and vaccines) will be discussed. Finally, future strategies to ameliorate the efficacy of immunotherapy and facilitate clinical translation will be provided to address the unmet medical needs of GBM.
Keywords: Brain cancer; Cancer vaccine; Combination immunotherapy; Glioblastoma; Immune checkpoint blockade.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Cloughesy TF, Cavenee WK, Mischel PS. Glioblastoma: from molecular pathology to targeted treatment. Annu Rev Pathol Mech Dis. 2014;9:1–25. - PubMed
-
- Wesseling P, Capper D. WHO 2016 classification of gliomas. Neuropathol Appl Neurobiol. 2018;44:139–150. - PubMed
-
- Fan X, Xiong Y, Wang Y. A reignited debate over the cell(s) of origin for glioblastoma and its clinical implications. Front Med. 2019;13:531–539. - PubMed
-
- Ohgaki H, Kleihues P. The definition of primary and secondary glioblastoma. Clin Cancer Res. 2013;19:764–772. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
