

Enhanced oxidative stress and presence of ventricular aneurysm for risk prediction in cardiac sarcoidosis
- PMID: 35078868
- PMCID: PMC8899481
- DOI: 10.1136/heartjnl-2021-320244
Enhanced oxidative stress and presence of ventricular aneurysm for risk prediction in cardiac sarcoidosis
Abstract
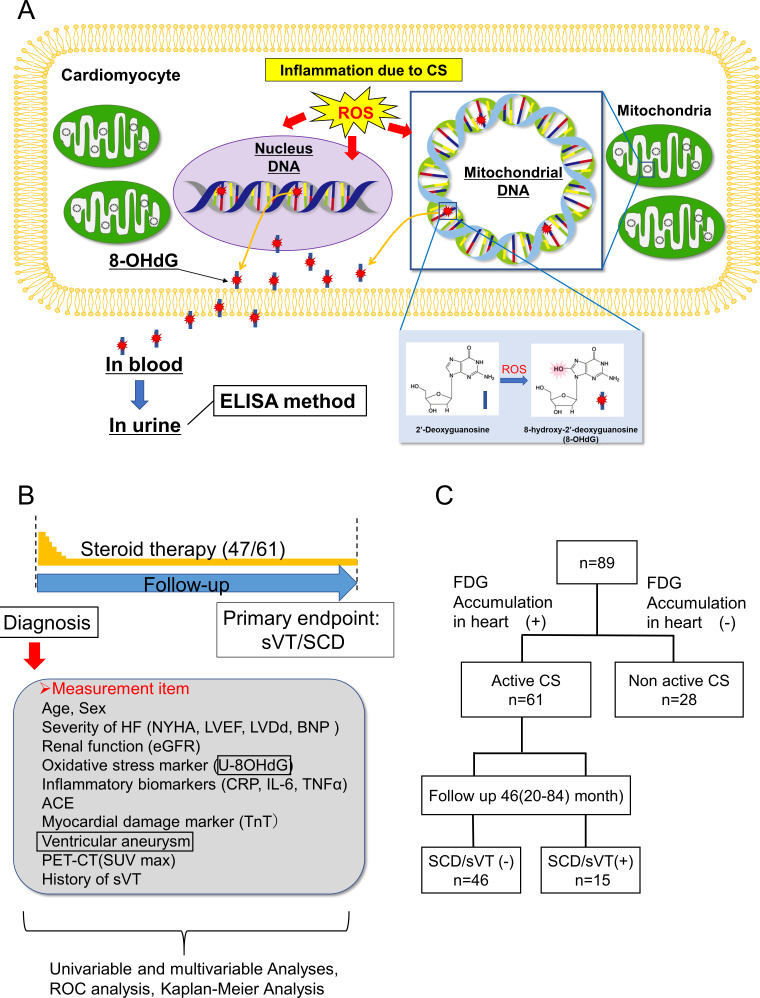
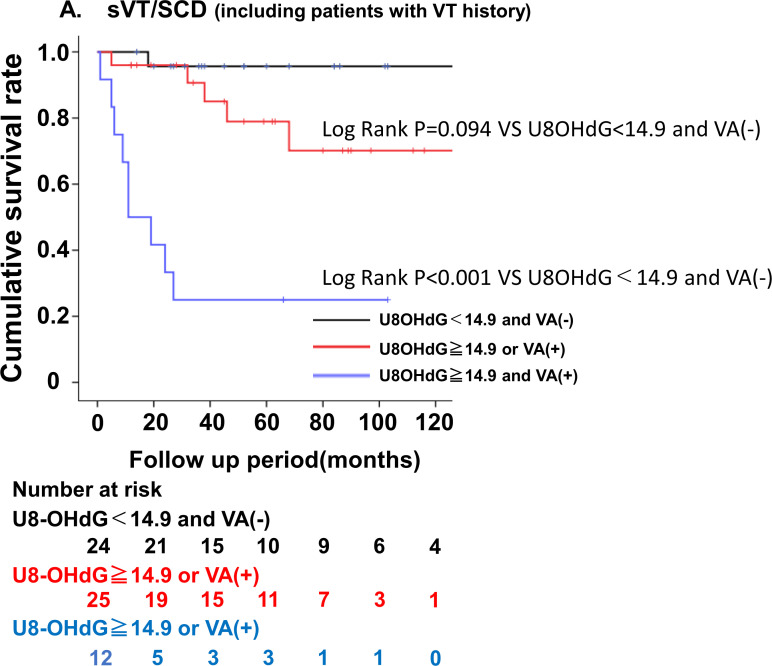
Objective: Sudden cardiac death (SCD) is the major cause of death in cardiac sarcoidosis (CS). We aimed to identify the prognostic markers for sustained ventricular tachycardia (sVT) and SCD in patients with CS.
Methods: We performed a prospective observational cohort study for patients with CS diagnosed according to the Japanese or Heart Rhythm Society guidelines between June 2008 and March 2020 in our hospital. The primary endpoint was a composite of the first sVT and SCD. The levels of urinary 8-hydroxy-2'-deoxyguanosine (U-8-OHdG), a marker of oxidative DNA damage that reflects the inflammatory activity of CS, other biomarkers, and indices of cardiac function and renal function were measured on admission.
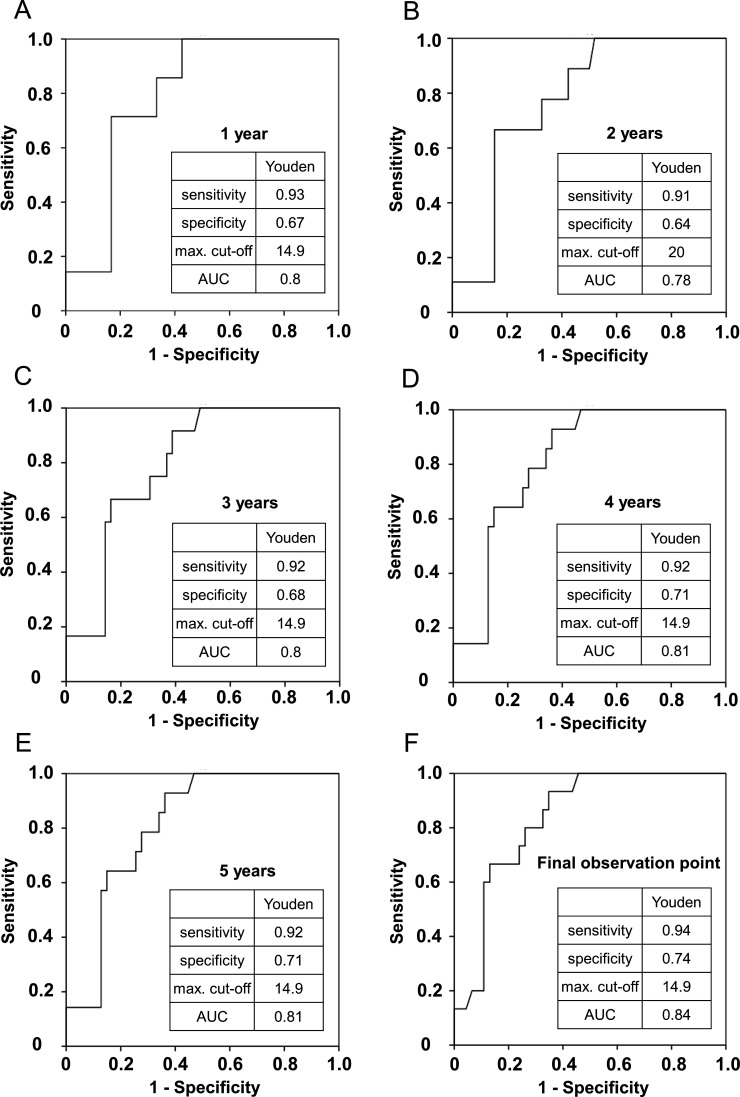
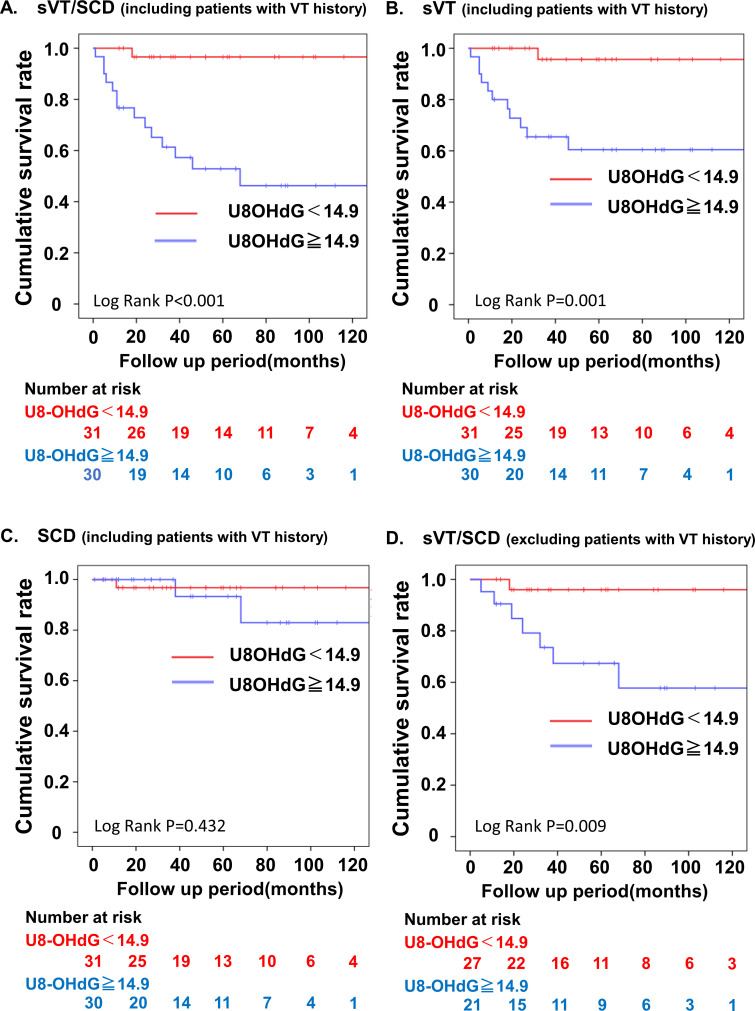
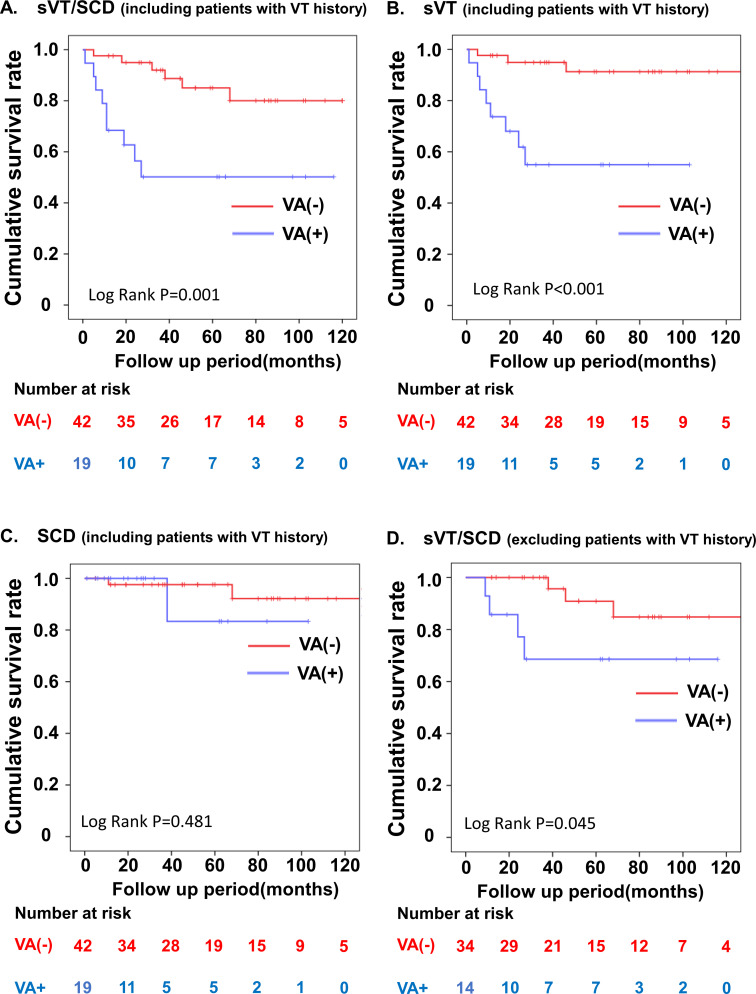
Results: Eighty-nine consecutive patients with CS were enrolled; 28 patients with no abnormal 18F-fluorodeoxyglucose (18F-FDG) accumulation in the heart were excluded and 61 patients with abnormal 18F-FDG accumulation were followed up for a median of 46 months (IQR: 20-84). During the follow-up period, 15 of 61 patients showed sVT (n=12) or SCD (n=3). A Cox proportional hazard model showed that U-8-OHdG concentration and presence of ventricular aneurysm (VA) were independent predictors of first sVT/SCD. The cut-off U-8-OHdG concentration for predicting first sVT/SCD was 14.9 ng/mg·Cr. Patients with U-8-OHdG concentration ≥14.9 ng/mg·Cr and VA showed a significantly increased risk of sVT/SCD.
Conclusions: U-8-OHdG and presence of VA were powerful predictors of first sVT/SCD in patients with CS, facilitating the stratification of cardiac events and providing relevant information about the substrates of ventricular tachycardia.
Keywords: biomarkers; cardiomyopathies; tachycardia; ventricular.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Cardiac oxidative stress: a potential tool for risk stratification in cardiac sarcoidosis.Heart. 2022 Mar;108(6):410-411. doi: 10.1136/heartjnl-2021-320590. Epub 2022 Jan 25. Heart. 2022. PMID: 35078869 No abstract available.
References
-
- Zipse MM, Tzou WS, Schuller JL, et al. . Electrophysiologic testing for diagnostic evaluation and risk stratification in patients with suspected cardiac sarcoidosis with preserved left and right ventricular systolic function. J Cardiovasc Electrophysiol 2019;30:1939–48. 10.1111/jce.14058 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical