

Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome
- PMID: 35078982
- PMCID: PMC8789854
- DOI: 10.1038/s41467-021-27797-1
Immunoglobulin signature predicts risk of post-acute COVID-19 syndrome
Abstract
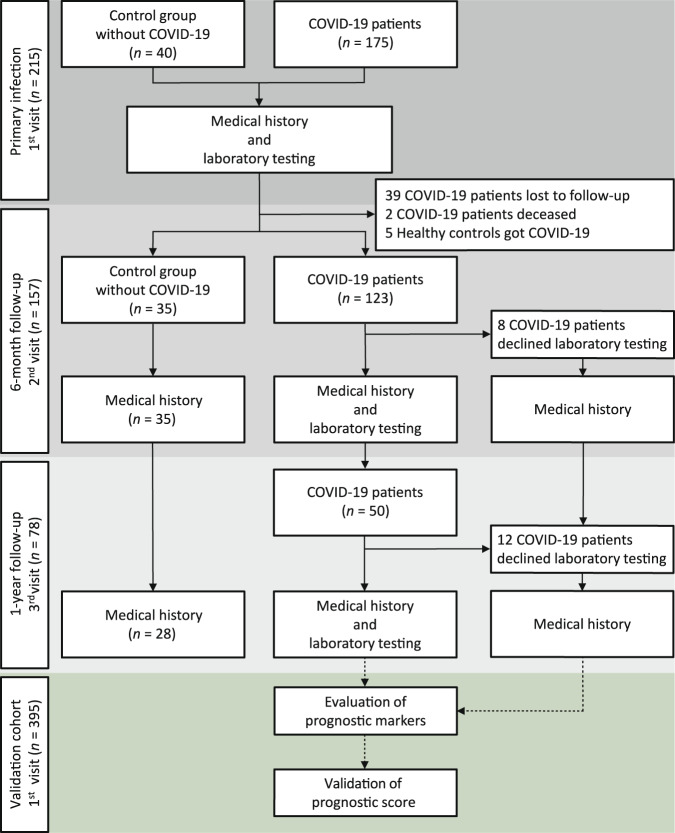
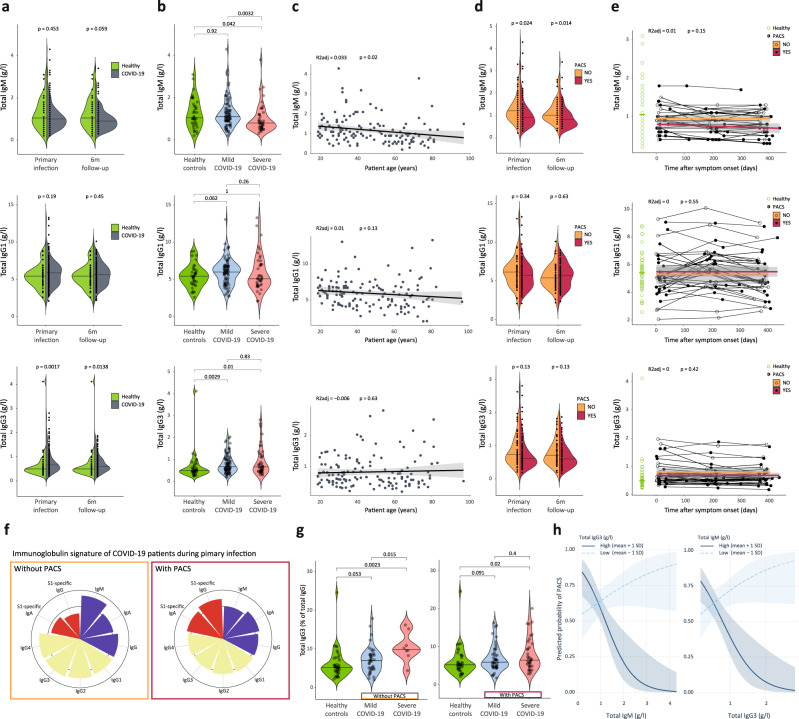
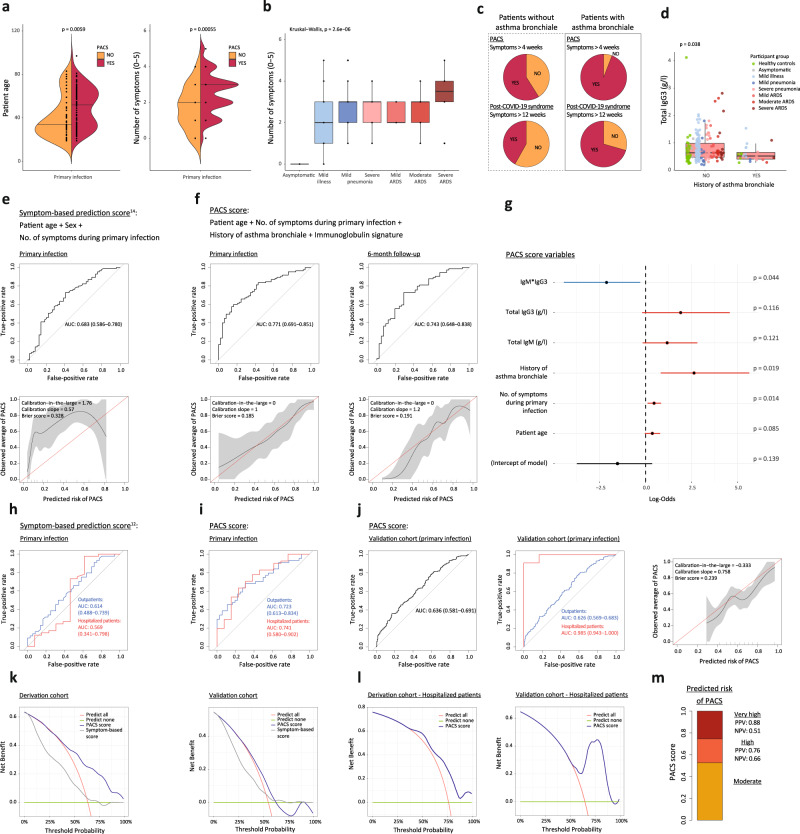
Following acute infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) a significant proportion of individuals develop prolonged symptoms, a serious condition termed post-acute coronavirus disease 2019 (COVID-19) syndrome (PACS) or long COVID. Predictors of PACS are needed. In a prospective multicentric cohort study of 215 individuals, we study COVID-19 patients during primary infection and up to one year later, compared to healthy subjects. We discover an immunoglobulin (Ig) signature, based on total IgM and IgG3 levels, which - combined with age, history of asthma bronchiale, and five symptoms during primary infection - is able to predict the risk of PACS independently of timepoint of blood sampling. We validate the score in an independent cohort of 395 individuals with COVID-19. Our results highlight the benefit of measuring Igs for the early identification of patients at high risk for PACS, which facilitates the study of targeted treatment and pathomechanisms of PACS.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- NRP 78 Implementation Programme/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- 4078P0-198431/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- NRP 78 Implementation Programme/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- 4078P0-198431/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- 310030-200669/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)
- 323530-191220/Schweizerische Akademie der Medizinischen Wissenschaften (Swiss Academy of Medical Sciences)
- 323530-191230/Schweizerische Akademie der Medizinischen Wissenschaften (Swiss Academy of Medical Sciences)
- 323530-177975/Schweizerische Akademie der Medizinischen Wissenschaften (Swiss Academy of Medical Sciences)
- YTCR 32/18/Schweizerische Akademie der Medizinischen Wissenschaften (Swiss Academy of Medical Sciences)
- YTCR 32/18/Gottfried und Julia Bangerter-Rhyner-Stiftung (Bangerter-Stiftung)
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
