

Assessment of fluid unresponsiveness guided by lung ultrasound in abdominal surgery: a prospective cohort study
- PMID: 35079044
- PMCID: PMC8789825
- DOI: 10.1038/s41598-022-05251-6
Assessment of fluid unresponsiveness guided by lung ultrasound in abdominal surgery: a prospective cohort study
Abstract
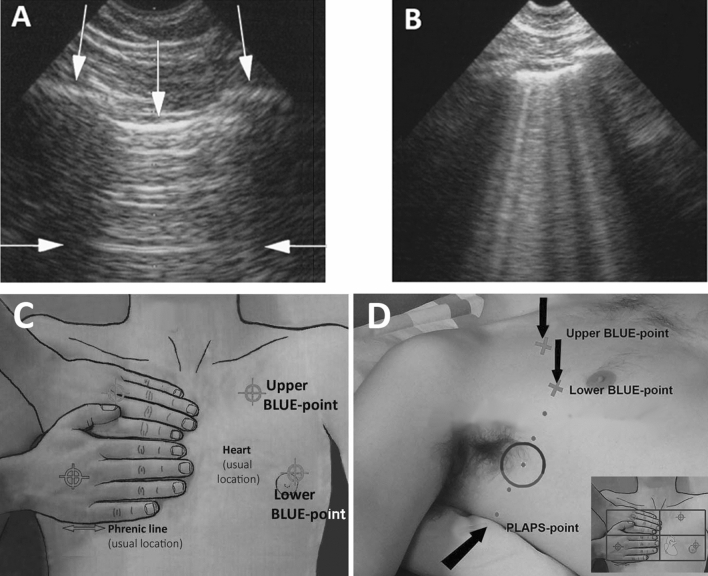
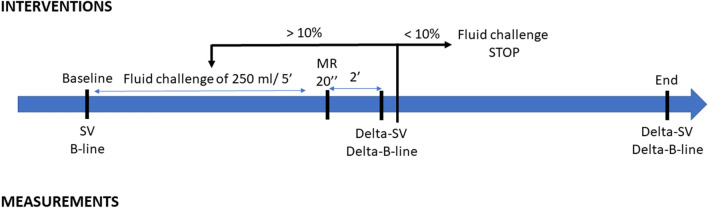
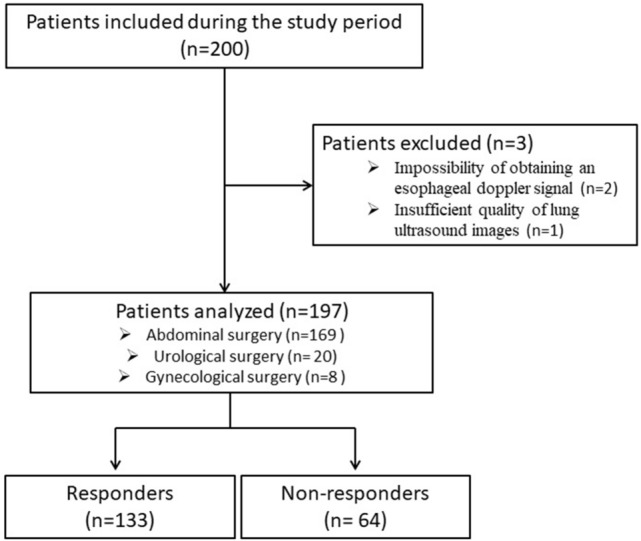
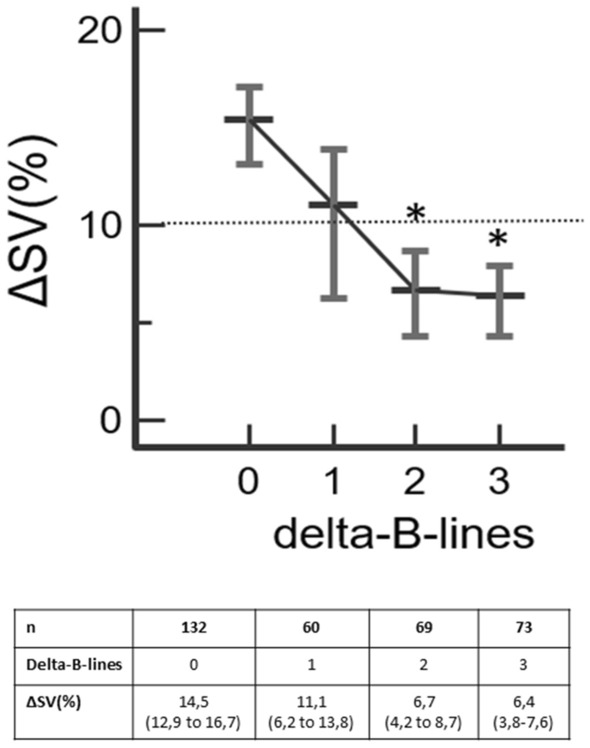
A fluid challenge can generate an infraclinical interstitial syndrome that may be detected by the appearance of B-lines by lung ultrasound. Our objective was to evaluate the appearance of B-lines as a diagnostic marker of preload unresponsiveness and postoperative complications in the operating theater. We conducted a prospective, bicentric, observational study. Adult patients undergoing abdominal surgery were included. Stroke volume (SV) was determined before and after a fluid challenge with 250 mL crystalloids (Delta-SV) using esophageal Doppler monitoring. Responders were defined by an increase of Delta-SV > 10% after fluid challenge. B-lines were collected at four bilateral predefined zones (right and left anterior and lateral). Delta-B-line was defined as the number of newly appearing B-lines after a fluid challenge. Postoperative pulmonary complications were prospectively recorded according to European guidelines. In total, 197 patients were analyzed. After a first fluid challenge, 67% of patients were responders and 33% were non-responders. Delta-B-line was significantly higher in non-responders than responders [4 (2-7) vs 1 (0-3), p < 0.0001]. Delta-B-line was able to diagnose fluid non-responders with an area under the curve of 0.74 (95% CI 0.67-0.80, p < 0.0001). The best threshold was two B-lines with a sensitivity of 80% and a specificity of 57%. The final Delta-B-line could predict postoperative pulmonary complications with an area under the curve of 0.74 (95% CI 0.67-0.80, p = 0.0004). Delta-B-line of two or more detected in four lung ultrasound zones can be considered to be a marker of preload unresponsiveness after a fluid challenge in abdominal surgery.The objectives and procedures of the study were registered at Clinicaltrials.gov (NCT03502460; Principal investigator: Stéphane BAR, date of registration: April 18, 2018).
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
