

Automatic segmentation of high-risk clinical target volume for tandem-and-ovoids brachytherapy patients using an asymmetric dual-path convolutional neural network
- PMID: 35080018
- PMCID: PMC9170543
- DOI: 10.1002/mp.15490
Automatic segmentation of high-risk clinical target volume for tandem-and-ovoids brachytherapy patients using an asymmetric dual-path convolutional neural network
Abstract
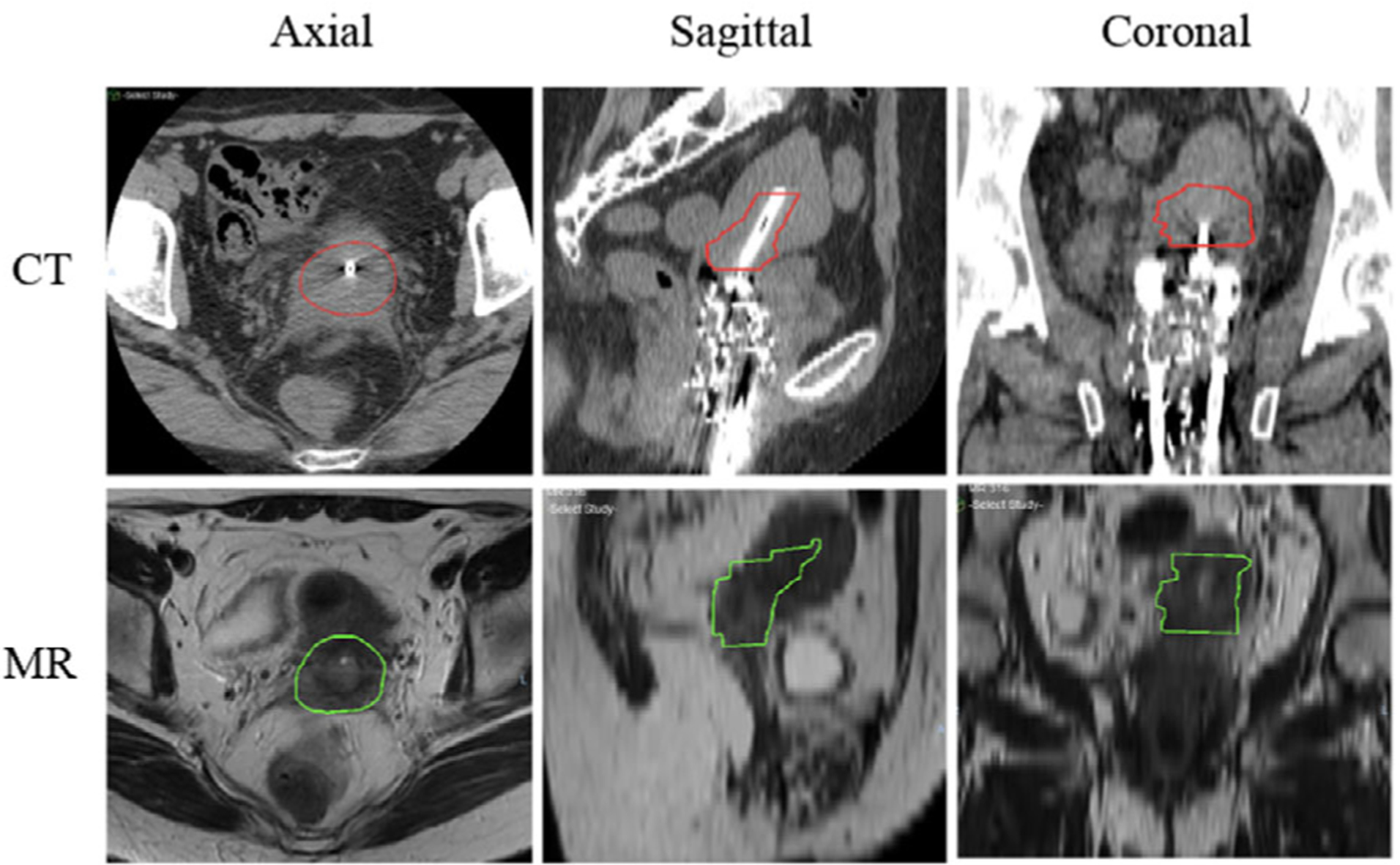
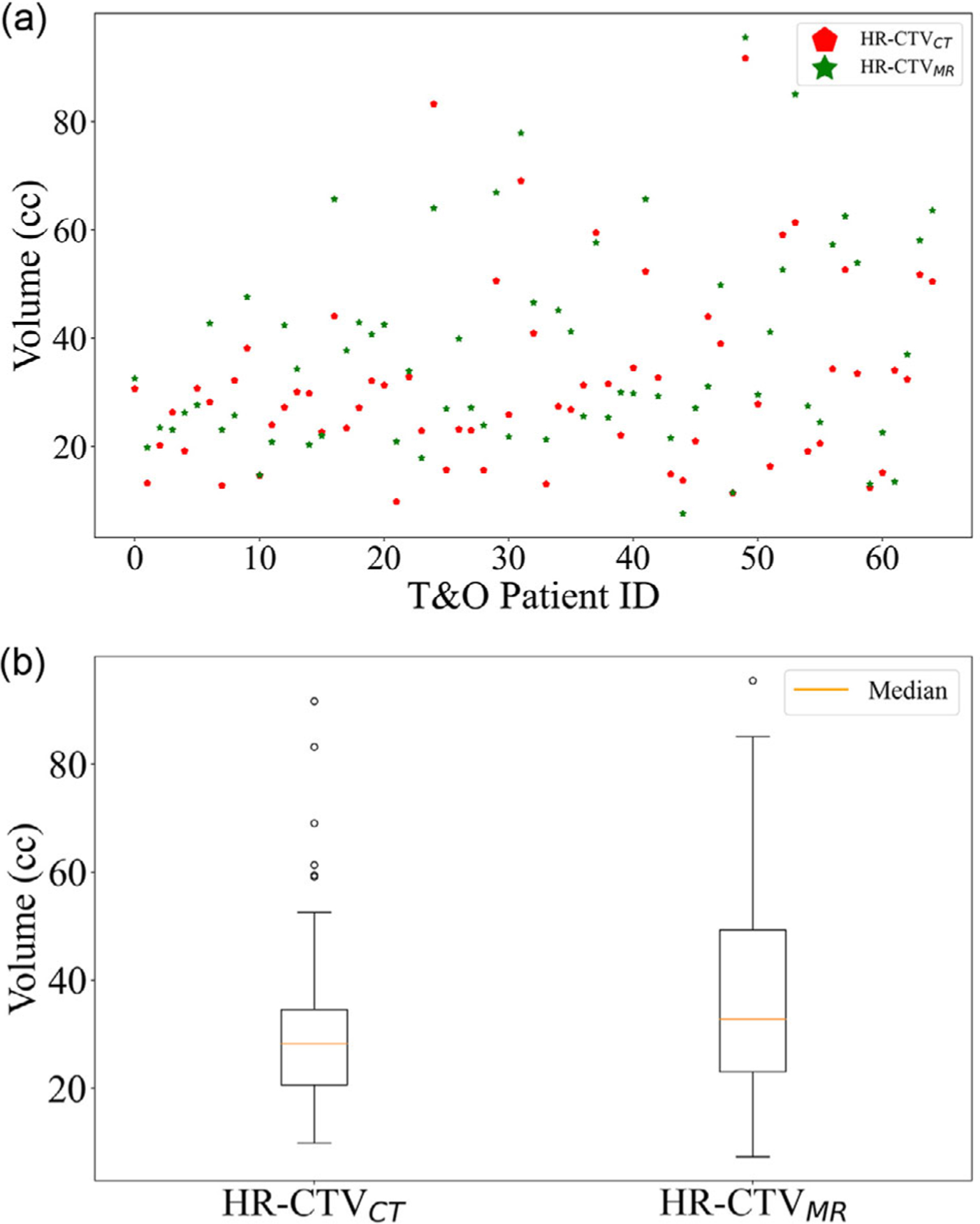
Purposes: Preimplant diagnostic magnetic resonance imaging is the gold standard for image-guided tandem-and-ovoids (T&O) brachytherapy for cervical cancer. However, high dose rate brachytherapy planning is typically done on postimplant CT-based high-risk clinical target volume (HR-CTVCT ) because the transfer of preimplant Magnetic resonance (MR)-based HR-CTV (HR-CTVMR ) to the postimplant planning CT is difficult due to anatomical changes caused by applicator insertion, vaginal packing, and the filling status of the bladder and rectum. This study aims to train a dual-path convolutional neural network (CNN) for automatic segmentation of HR-CTVCT on postimplant planning CT with guidance from preimplant diagnostic MR.
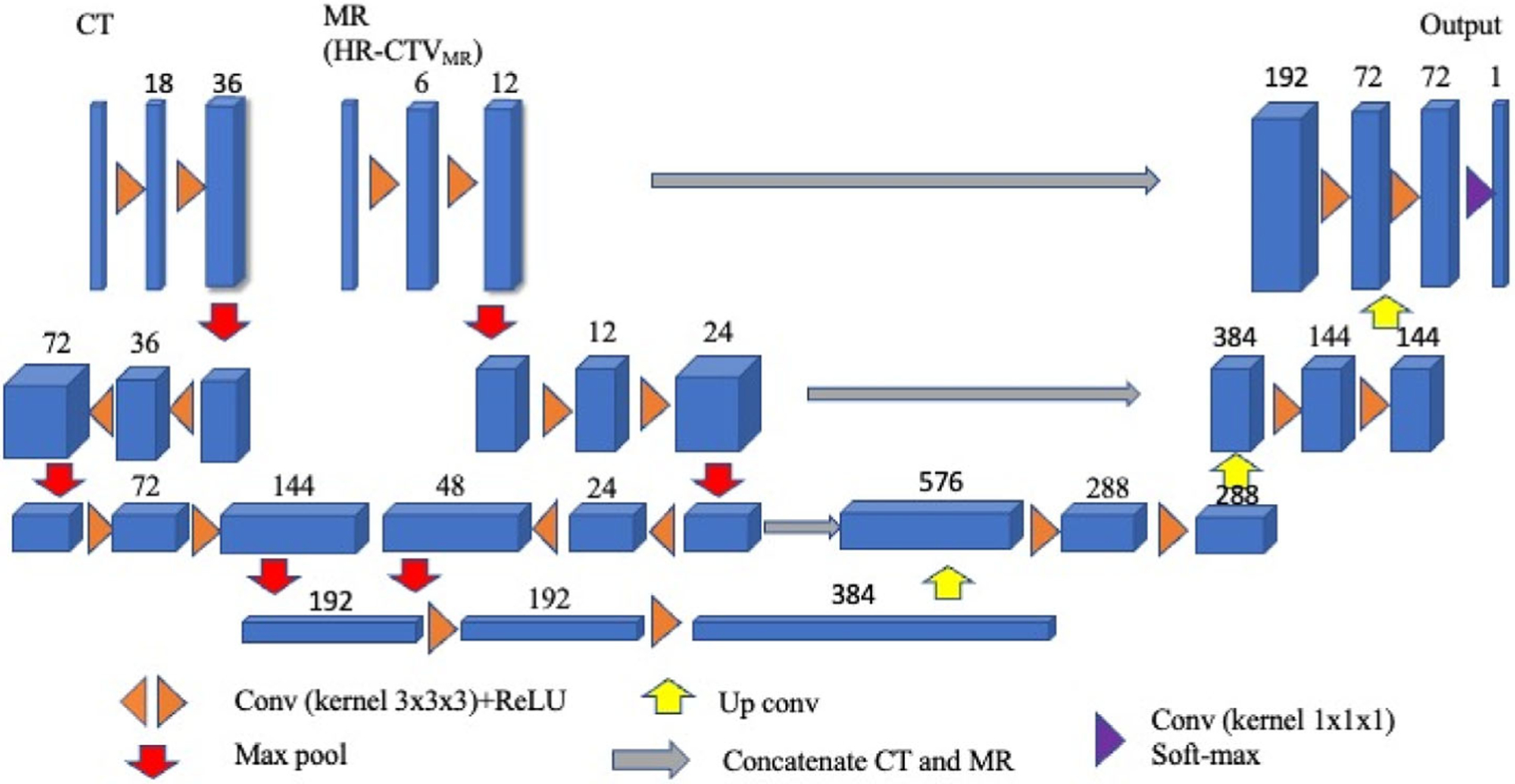
Methods: Preimplant T2-weighted MR and postimplant CT images for 65 (48 for training, eight for validation, and nine for testing) patients were retrospectively solicited from our institutional database. MR was aligned to the corresponding CT using rigid registration. HR-CTVCT and HR-CTVMR were manually contoured on CT and MR by an experienced radiation oncologist. All images were then resampled to a spatial resolution of 0.5 × 0.5 × 1.25 mm. A dual-path 3D asymmetric CNN architecture with two encoding paths was built to extract CT and MR image features. The MR was masked by HR-CTVMR contour while the entire CT volume was included. The network put an asymmetric weighting of 18:6 for CT: MR. Voxel-based dice similarity coefficient (DSCV ), sensitivity, precision, and 95% Hausdorff distance (95-HD) were used to evaluate model performance. Cross-validation was performed to assess model stability. The study cohort was divided into a small tumor group (<20 cc), medium tumor group (20-40 cc), and large tumor group (>40 cc) based on the HR-CTVCT for model evaluation. Single-path CNN models were trained with the same parameters as those in dual-path models.
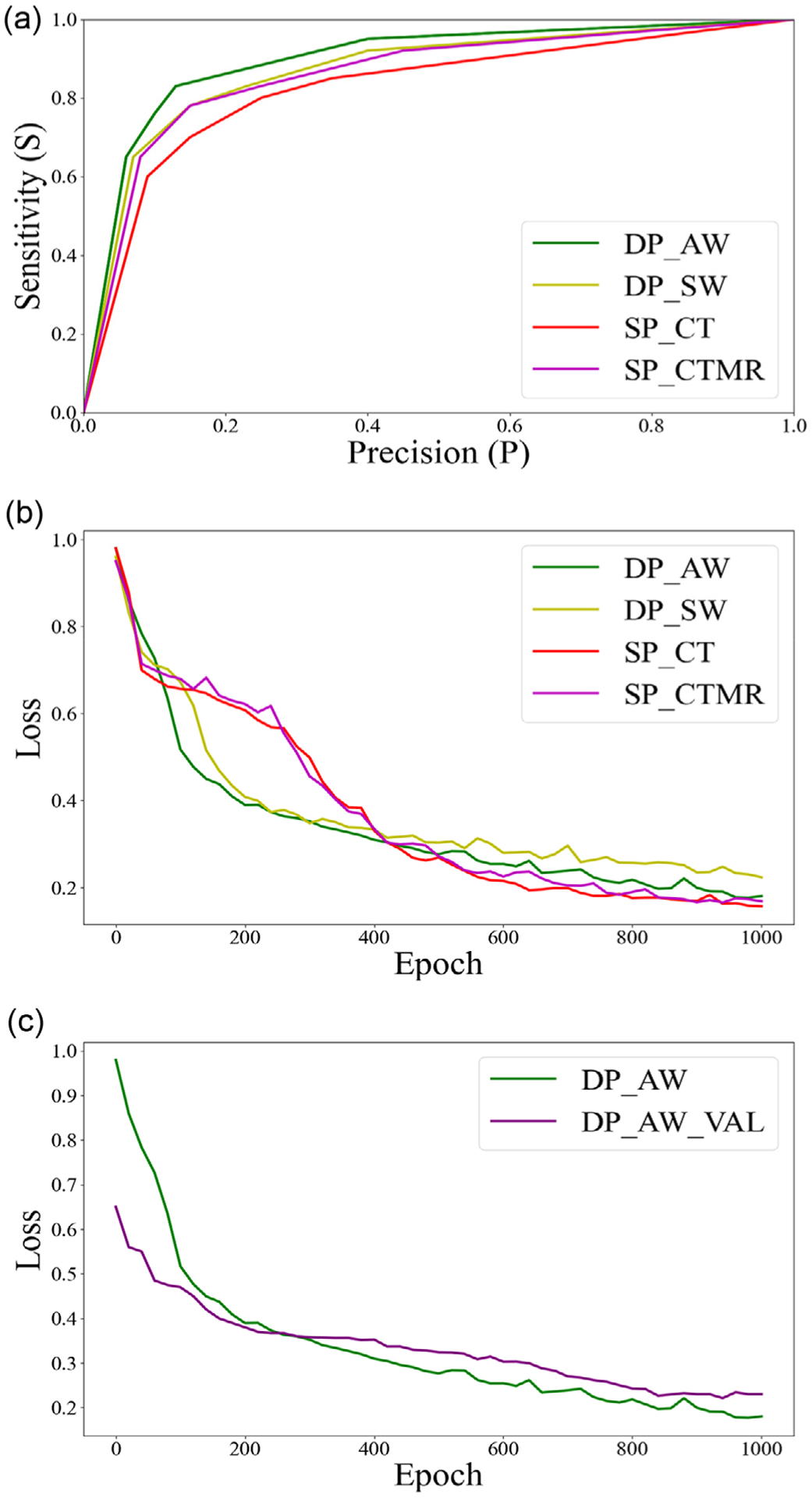
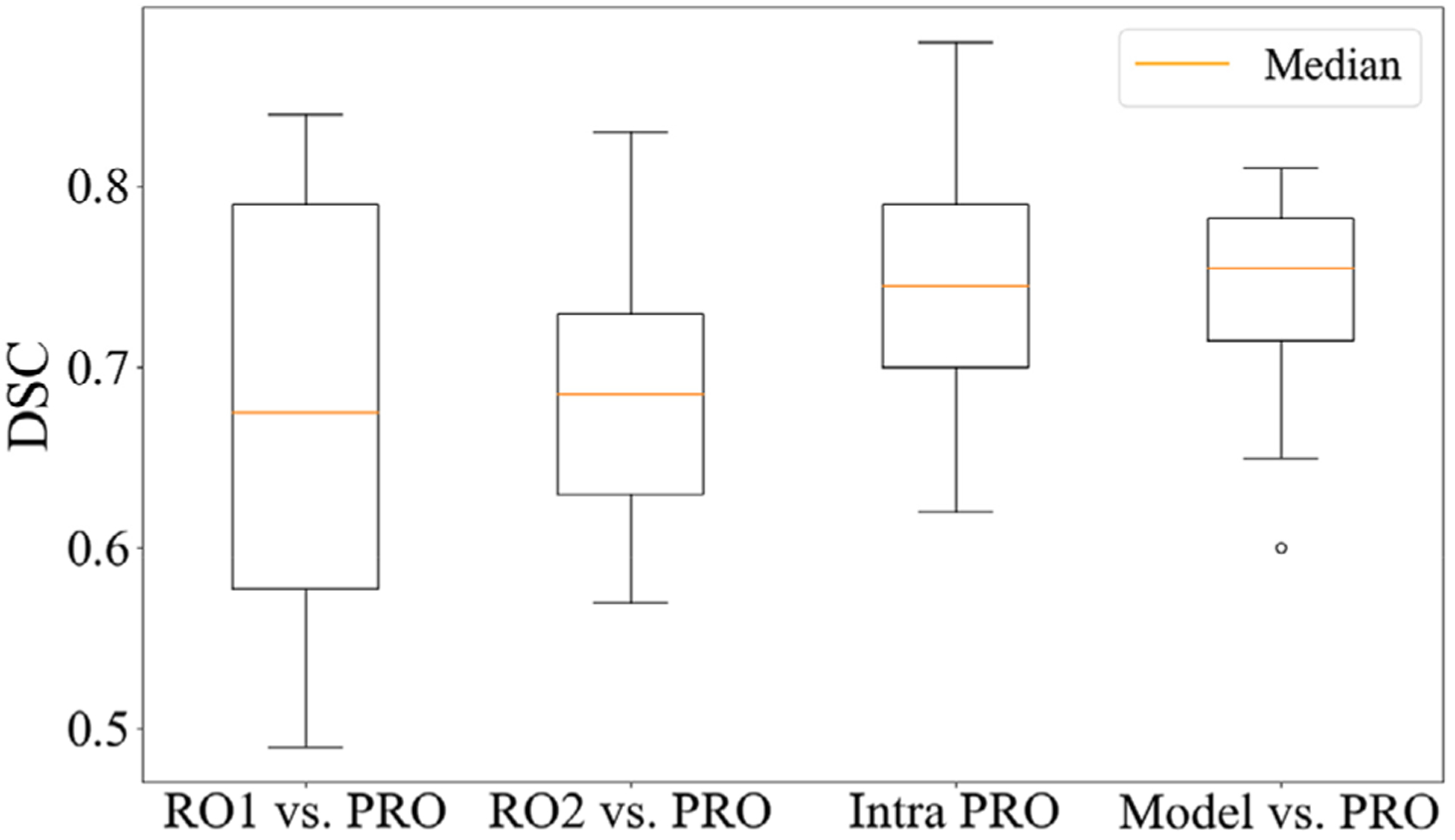
Results: For this patient cohort, the dual-path CNN model improved each of our objective findings, including DSCV , sensitivity, and precision, with an average improvement of 8%, 7%, and 12%, respectively. The 95-HD was improved by an average of 1.65 mm compared to the single-path model with only CT images as input. In addition, the area under the curve for different networks was 0.86 (dual-path with CT and MR) and 0.80 (single-path with CT), respectively. The dual-path CNN model with asymmetric weighting achieved the best performance with DSCV of 0.65 ± 0.03 (0.61-0.70), 0.79 ± 0.02 (0.74-0.85), and 0.75 ± 0.04 (0.68-0.79) for small, medium, and large group. 95-HD were 7.34 (5.35-10.45) mm, 5.48 (3.21-8.43) mm, and 6.21 (5.34-9.32) mm for the three size groups, respectively.
Conclusions: An asymmetric CNN model with two encoding paths from preimplant MR (masked by HR-CTVMR ) and postimplant CT images was successfully developed for automatic segmentation of HR-CTVCT for T&O brachytherapy patients.
Keywords: CNN; Deep learning; HDR; Tandem and Ovoids; high-risk CTV; segmentation.
© 2022 American Association of Physicists in Medicine.
Conflict of interest statement
CONFLICT OF INTEREST
The authors have no conflict of interest to disclose.
Figures
References
-
- Viswanathan AN, Thomadsen B. Committee ABSCCR. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part I: general principles. Brachytherapy. 2012;11:33–46. - PubMed
-
- Nomden CN, de Leeuw AA, Roesink JM, et al. Clinical outcome and dosimetric parameters of chemo-radiation including MRI guided adaptive brachytherapy with tandem-ovoid applicators for cervical cancer patients:a single institution experience. Radiother Oncol. 2013;107:69–74. - PubMed
-
- Haie-Meder C, Pötter R, Van Limbergen E, et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group☆(I): concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother Oncol.2005;74:235–245. - PubMed
