

Trajectories of Insomnia in Adults After Traumatic Brain Injury
- PMID: 35080600
- PMCID: PMC8792888
- DOI: 10.1001/jamanetworkopen.2021.45310
Trajectories of Insomnia in Adults After Traumatic Brain Injury
Abstract
Importance: Insomnia is common after traumatic brain injury (TBI) and contributes to morbidity and long-term sequelae.
Objective: To identify unique trajectories of insomnia in the 12 months after TBI.
Design, setting, and participants: In this prospective cohort study, latent class mixed models (LCMMs) were used to model insomnia trajectories over time and to classify participants into distinct profile groups. Data from the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study, a longitudinal, multisite, observational study, were uploaded to the Federal Interagency Traumatic Brain Injury Repository (FITBIR) database. Participants were enrolled at 1 of 18 participating level I trauma centers and enrolled within 24 hours of TBI injury. Additional data were obtained directly from the TRACK-TBI investigators that will be uploaded to FITBIR in the future. Data were collected from February 26, 2014, to August 8, 2018, and analyzed from July 1, 2020, to November 15, 2021.
Exposures: Traumatic brain injury.
Main outcomes and measures: Insomnia Severity Index assessed serially at 2 weeks and 3, 6, and 12 months thereafter.
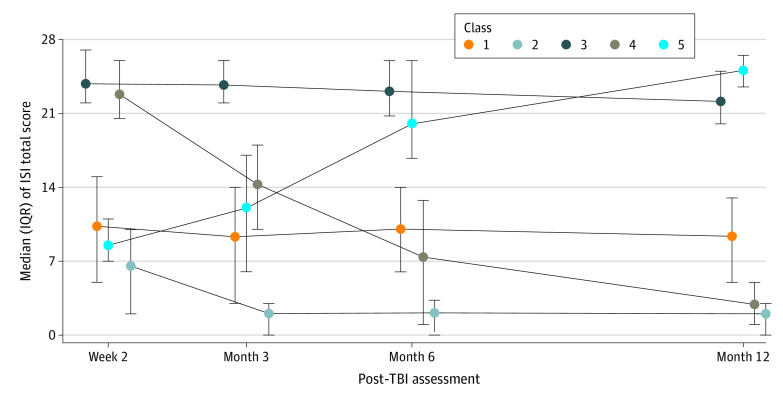
Results: The final sample included 2022 participants (1377 [68.1%] men; mean [SD] age, 40.1 [17.2] years) from the FITBIR database and the TRACK-TBI study. The data were best fit by a 5-class LCMM. Of these participants, 1245 (61.6%) reported persistent mild insomnia symptoms (class 1); 627 (31.0%) initially reported mild insomnia symptoms that resolved over time (class 2); 91 (4.5%) reported persistent severe insomnia symptoms (class 3); 44 (2.2%) initially reported severe insomnia symptoms that resolved by 12 months (class 4); and 15 (0.7%) initially reported no insomnia symptoms but had severe symptoms by 12 months (class 5). In a multinomial logistic regression model, several factors significantly associated with insomnia trajectory class membership were identified, including female sex (odds ratio [OR], 1.65 [95% CI, 1.02-2.66]), Black race (OR, 2.36 [95% CI, 1.39-4.01]), history of psychiatric illness (OR, 2.21 [95% CI, 1.35-3.60]), and findings consistent with intracranial injury on computed tomography (OR, 0.36 [95% CI, 0.20-0.65]) when comparing class 3 with class 1.
Conclusions and relevance: These results suggest important heterogeneity in the course of insomnia after TBI in adults. More work is needed to identify outcomes associated with these insomnia trajectory class subgroups and to identify optimal subgroup-specific treatment approaches.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
