Autonomous robotic laparoscopic surgery for intestinal anastomosis
- PMID: 35080901
- PMCID: PMC8992572
- DOI: 10.1126/scirobotics.abj2908
Autonomous robotic laparoscopic surgery for intestinal anastomosis
Abstract
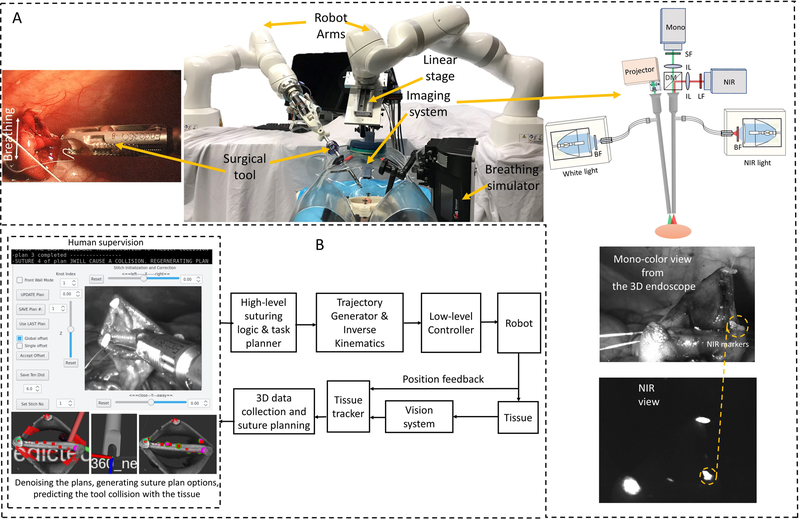
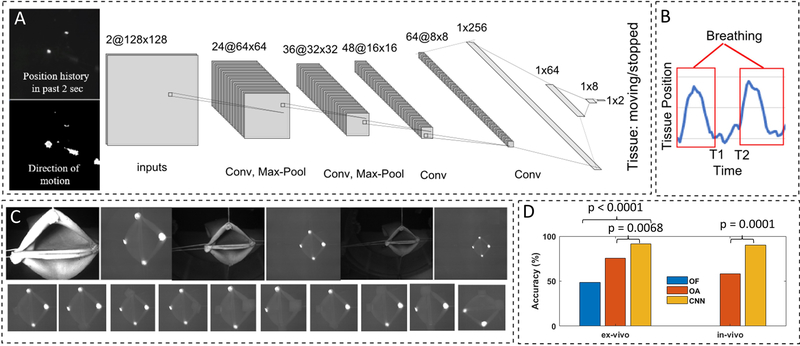
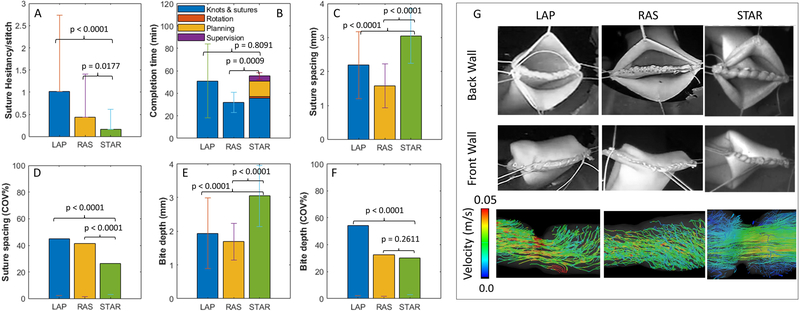
Autonomous robotic surgery has the potential to provide efficacy, safety, and consistency independent of individual surgeon's skill and experience. Autonomous anastomosis is a challenging soft-tissue surgery task because it requires intricate imaging, tissue tracking, and surgical planning techniques, as well as a precise execution via highly adaptable control strategies often in unstructured and deformable environments. In the laparoscopic setting, such surgeries are even more challenging because of the need for high maneuverability and repeatability under motion and vision constraints. Here we describe an enhanced autonomous strategy for laparoscopic soft tissue surgery and demonstrate robotic laparoscopic small bowel anastomosis in phantom and in vivo intestinal tissues. This enhanced autonomous strategy allows the operator to select among autonomously generated surgical plans and the robot executes a wide range of tasks independently. We then use our enhanced autonomous strategy to perform in vivo autonomous robotic laparoscopic surgery for intestinal anastomosis on porcine models over a 1-week survival period. We compared the anastomosis quality criteria-including needle placement corrections, suture spacing, suture bite size, completion time, lumen patency, and leak pressure-of the developed autonomous system, manual laparoscopic surgery, and robot-assisted surgery (RAS). Data from a phantom model indicate that our system outperforms expert surgeons' manual technique and RAS technique in terms of consistency and accuracy. This was also replicated in the in vivo model. These results demonstrate that surgical robots exhibiting high levels of autonomy have the potential to improve consistency, patient outcomes, and access to a standard surgical technique.
Conflict of interest statement
Figures
Comment in
-
Autonomous robotic surgery makes light work of anastomosis.Sci Robot. 2022 Jan 26;7(62):eabn6522. doi: 10.1126/scirobotics.abn6522. Epub 2022 Jan 26. Sci Robot. 2022. PMID: 35080900
-
Autonomous robotic laparoscopic gastrointestinal surgery.Nat Rev Gastroenterol Hepatol. 2022 Mar;19(3):148. doi: 10.1038/s41575-022-00584-z. Nat Rev Gastroenterol Hepatol. 2022. PMID: 35105955 No abstract available.
References
-
- Rose PT, Nusbaum B, Robotic hair restoration, Dermatologic clinics 32, 97–107 (2014). - PubMed
-
- Perry TS, Profile: veebot [Resources_Start-ups], IEEE Spectrum 50, 23–23 (2013).
-
- Kilby W, Dooley JR, Kuduvalli G, Sayeh S, Maurer CR Jr, The CyberKnife® robotic radiosurgery system in 2010, Technology in cancer research & treatment 9, 433–452 (2010). - PubMed
-
- Haidegger T, Autonomy for Surgical Robots: Concepts and Paradigms, IEEE Transactions on Medical Robotics and Bionics 1, 65–76 (2019).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources