

Follow-up of patients with R/R FLT3-mutation-positive AML treated with gilteritinib in the phase 3 ADMIRAL trial
- PMID: 35081255
- PMCID: PMC9197557
- DOI: 10.1182/blood.2021011583
Follow-up of patients with R/R FLT3-mutation-positive AML treated with gilteritinib in the phase 3 ADMIRAL trial
Abstract
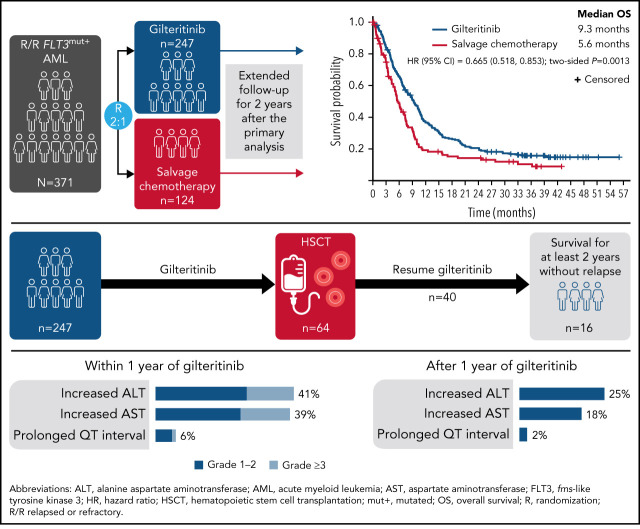
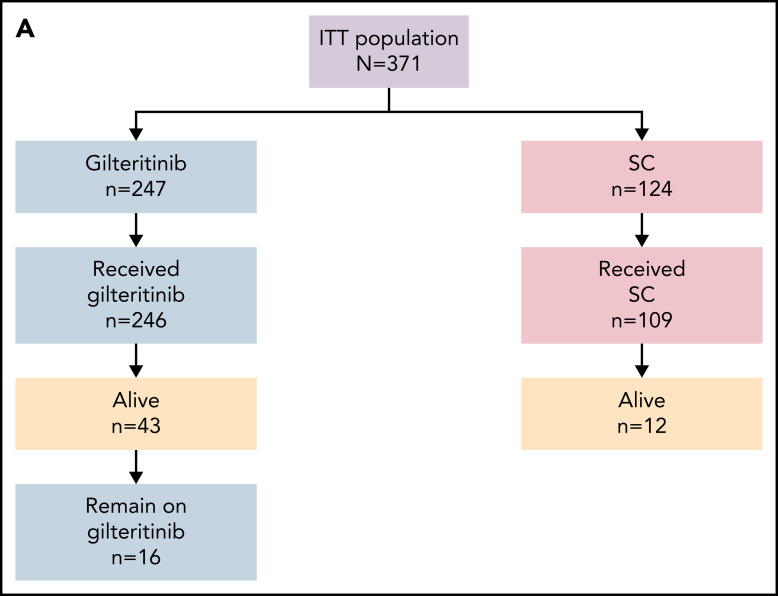
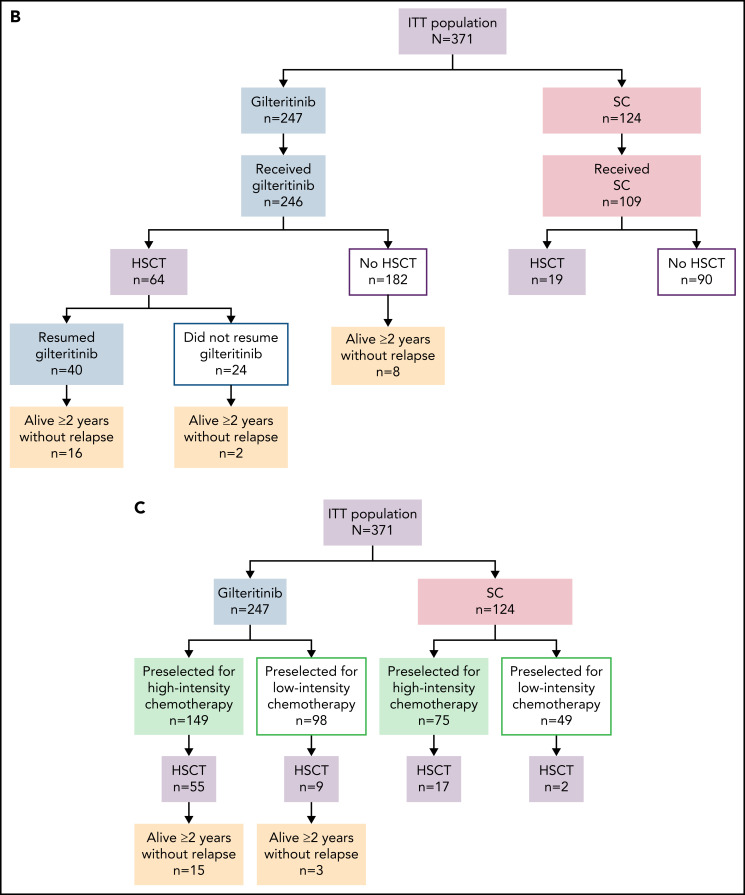
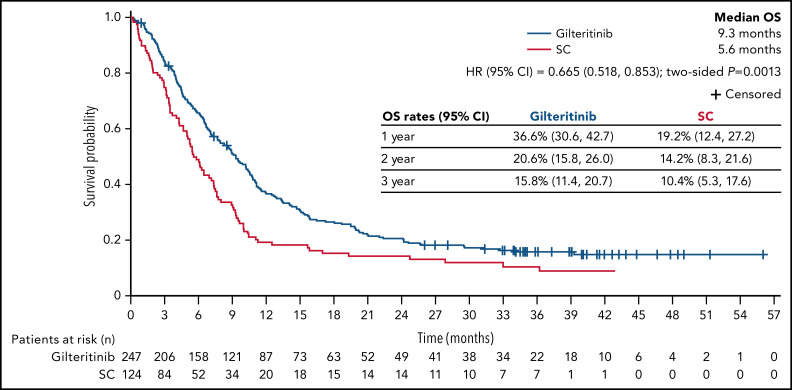
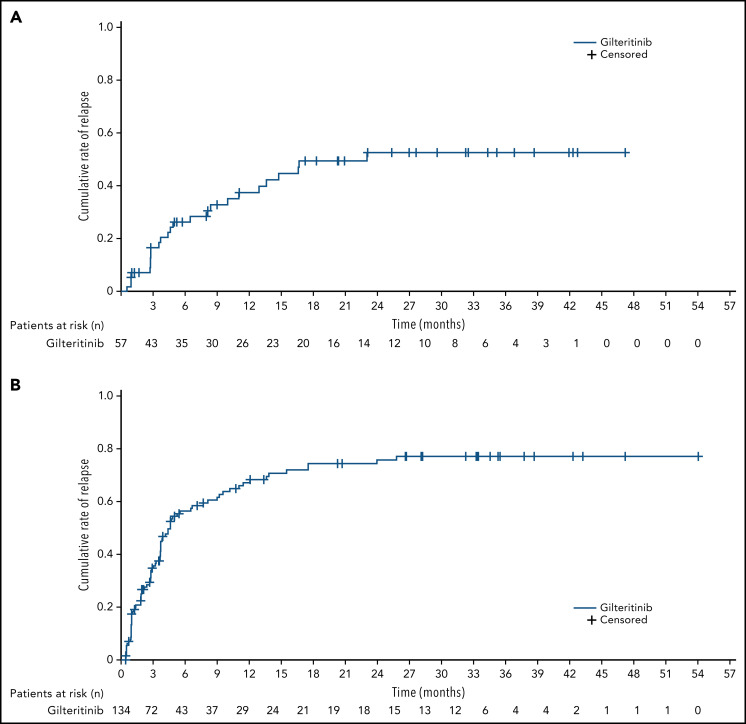
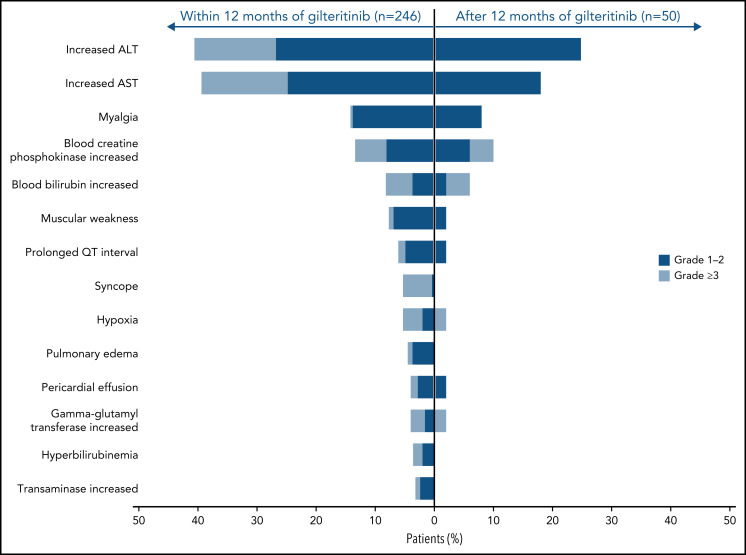
The phase 3 ADMIRAL (NCT02421939; Study ID: 2215-CL-0301) trial showed superior overall survival in patients with relapsed/refractory FLT3-mutation-positive acute myeloid leukemia (AML) randomized 2:1 to receive the oral FMS-like tyrosine kinase 3 inhibitor gilteritinib vs those randomized to receive salvage chemotherapy (SC). Here we provide a follow-up of the ADMIRAL trial 2 years after the primary analysis to clarify the long-term treatment effects and safety of gilteritinib in these patients with AML. At the time of this analysis, the median survival follow-up was 37.1 months, with deaths in 203 of 247 and 97 of 124 patients in the gilteritinib and SC arms, respectively; 16 gilteritinib-treated patients remained on treatment. The median overall survival for the gilteritinib and SC arms was 9.3 and 5.6 months, respectively (hazard ratio, 0.665; 95% confidence interval [CI], 0.518, 0.853; two-sided P = .0013); 2-year estimated survival rates were 20.6% (95% CI, 15.8, 26.0) and 14.2% (95% CI, 8.3, 21.6). The gilteritinib-arm 2-year cumulative incidence of relapse after composite complete remission was 75.7%, with few relapses occurring after 18 months. Overall, 49 of 247 patients in the gilteritinib arm and 14 of 124 patients in the SC arm were alive for ≥2 years. Twenty-six gilteritinib-treated patients remained alive for ≥2 years without relapse; 18 of these patients underwent transplantation (hematopoietic stem cell transplantation [HSCT]) and 16 restarted gilteritinib as post-HSCT maintenance therapy. The most common adverse events of interest during years 1 and 2 of gilteritinib therapy were increased liver transaminase levels; adverse event incidence decreased in year 2. Thus, continued and post-HSCT gilteritinib maintenance treatment sustained remission with a stable safety profile. These findings confirm that prolonged gilteritinib therapy is safe and is associated with superior survival vs SC. This trial was registered at www.clinicaltrials.gov as #NCT02421939.
© 2022 by The American Society of Hematology.
Figures
References
-
- Perl AE, Martinelli G, Cortes JE, et al. . Gilteritinib or chemotherapy for relapsed or refractory FLT3-mutated AML. N Engl J Med. 2019;381(18):1728-1740. - PubMed
-
- Cortes JE, Khaled S, Martinelli G, et al. . Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukaemia (QuANTUM-R): a multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):984-997. - PubMed
-
- DiNardo CD, Stein EM, de Botton S, et al. . Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Engl J Med. 2018;378(25):2386-2398. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
