

Ethnic/Racial Disparities in Longitudinal Neurocognitive Decline in People With HIV
- PMID: 35081558
- PMCID: PMC8986565
- DOI: 10.1097/QAI.0000000000002922
Ethnic/Racial Disparities in Longitudinal Neurocognitive Decline in People With HIV
Abstract
Background: To examine longitudinal neurocognitive decline among Latino, non-Latino Black, and non-Latino White people with HIV (PWH) and factors that may explain ethnic/racial disparities in neurocognitive decline.
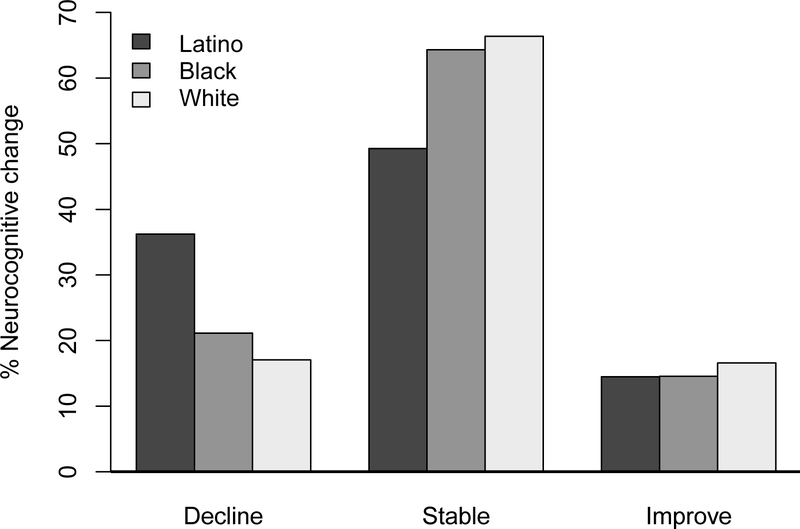
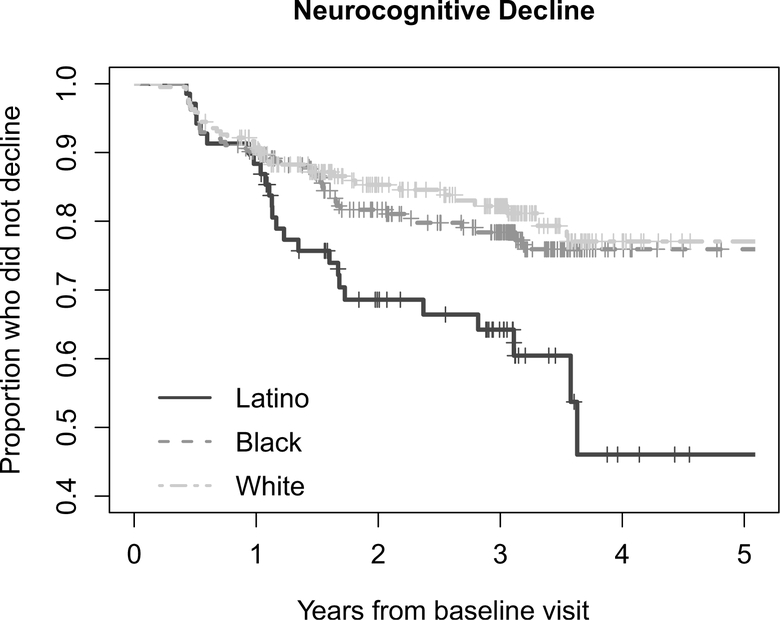
Methods: Four hundred ninety nine PWH (13.8% Latino, 42.7% Black, 43.5% White; baseline age: M = 43.5) from the CNS HIV Anti-Retroviral Therapy Effects Research (CHARTER) study completed neurocognitive, neuromedical, and laboratory assessments every 6-12 months with up to 5 years of follow-up. Longitudinal neurocognitive change was determined via published regression-based norms. Survival analyses investigated the relationship between ethnicity/race and neurocognitive change, and baseline and time-dependent variables that may explain ethnic/racial disparities in neurocognitive decline, including socio-demographic, HIV-disease, medical, psychiatric, and substance use characteristics.
Results: In Cox proportional hazard models, hazard ratios for neurocognitive decline were increased for Latino compared with White PWH (HR = 2.25, 95% CI = 1.35 to 3.73, P = 0.002), and Latino compared with Black PWH (HR = 1.86, 95% CI = 1.14 to 3.04, P = 0.013), with no significant differences between Black and White PWH (P = 0.40). Comorbidities, including cardiometabolic factors and more severe neurocognitive comorbidity classification, accounted for 33.6% of the excess hazard for Latino compared with White PWH, decreasing the hazard ratio associated with Latino ethnicity (HR = 1.83, 95% CI = 1.06 to 3.16, P = 0.03), but did not fully account for elevated risk of decline.
Conclusions: Latino PWH may be at higher risk of early neurocognitive decline compared with Black and White PWH. Comorbidities accounted for some, but not all, of this increased risk among Latino PWH. Future research examining institutional, sociocultural, and biomedical factors, including structural discrimination and age-related biomarkers, may further explain the observed disparities.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- CDC. HIV Surveillance Report, 2018 (Updated). 2020.
-
- Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clinical infectious diseases. 2013;57(8):1164–1171. - PubMed
-
- Buchacz K, Baker R, Palella F, et al. Disparities in prevalence of key chronic diseases by gender and race/ethnicity among antiretroviral-treated HIV-infected adults in the US. Antiviral Therapy. 2013;18(1):65–75. - PubMed
-
- Rawlings MK, Masters HL. Comorbidities and challenges affecting African Americans with HIV infection. Journal of the National Medical Association. 2008;100(12):1477–1481. - PubMed
