

Prehospital low titer group O whole blood is feasible and safe: Results of a prospective randomized pilot trial
- PMID: 35081595
- PMCID: PMC9038638
- DOI: 10.1097/TA.0000000000003551
Prehospital low titer group O whole blood is feasible and safe: Results of a prospective randomized pilot trial
Abstract
Introduction: Low titer group O whole blood (LTOWB) resuscitation is increasingly common in both military and civilian settings. Data regarding the safety and efficacy of prehospital LTOWB remain limited.
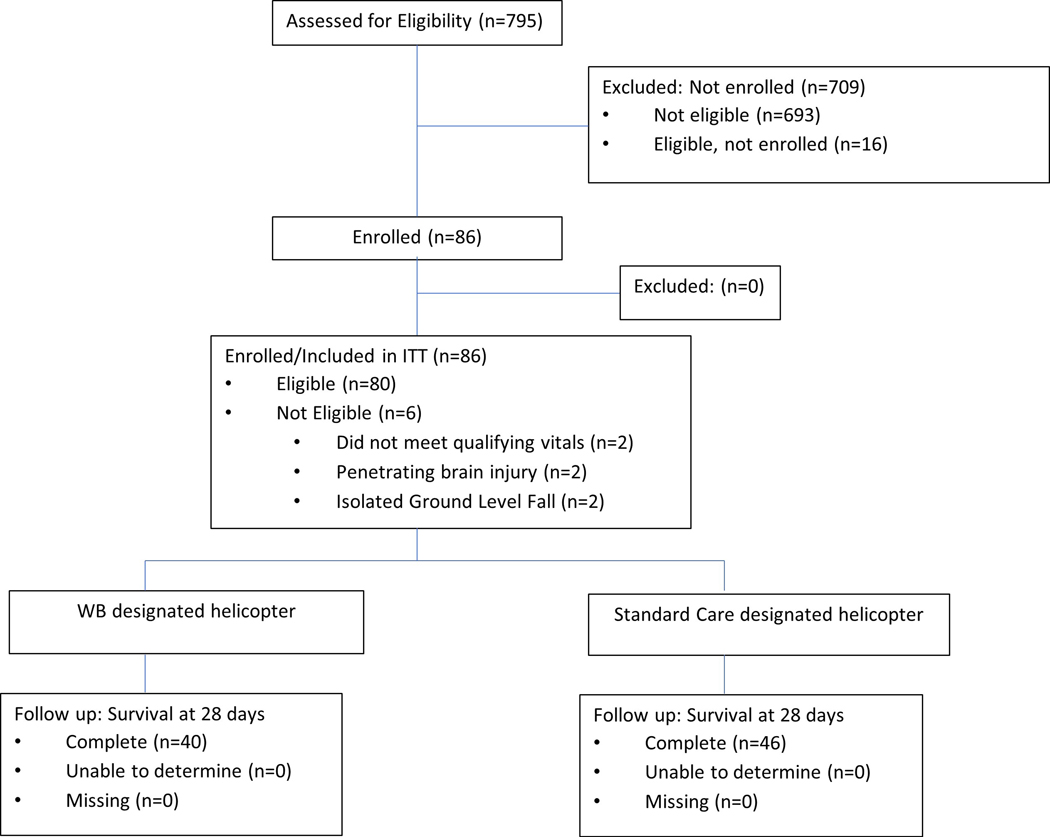
Methods: We performed a single-center, prospective, cluster randomized, prehospital through in-hospital whole blood pilot trial for injured air medical patients. We compared standard prehospital air medical care including red cell transfusion and crystalloids followed by in-hospital component transfusion to prehospital and in-hospital LTOWB resuscitation. Prehospital vital signs were used as inclusion criteria (systolic blood pressure ≤90 mm Hg and heart rate ≥108 beats per minute or systolic blood pressure ≤70 mm Hg for patients at risk of hemorrhage). Primary outcome was feasibility. Secondary outcomes included 28-day and 24-hour mortality, multiple organ failure, nosocomial infection, 24-hour transfusion requirements, and arrival coagulation parameters.
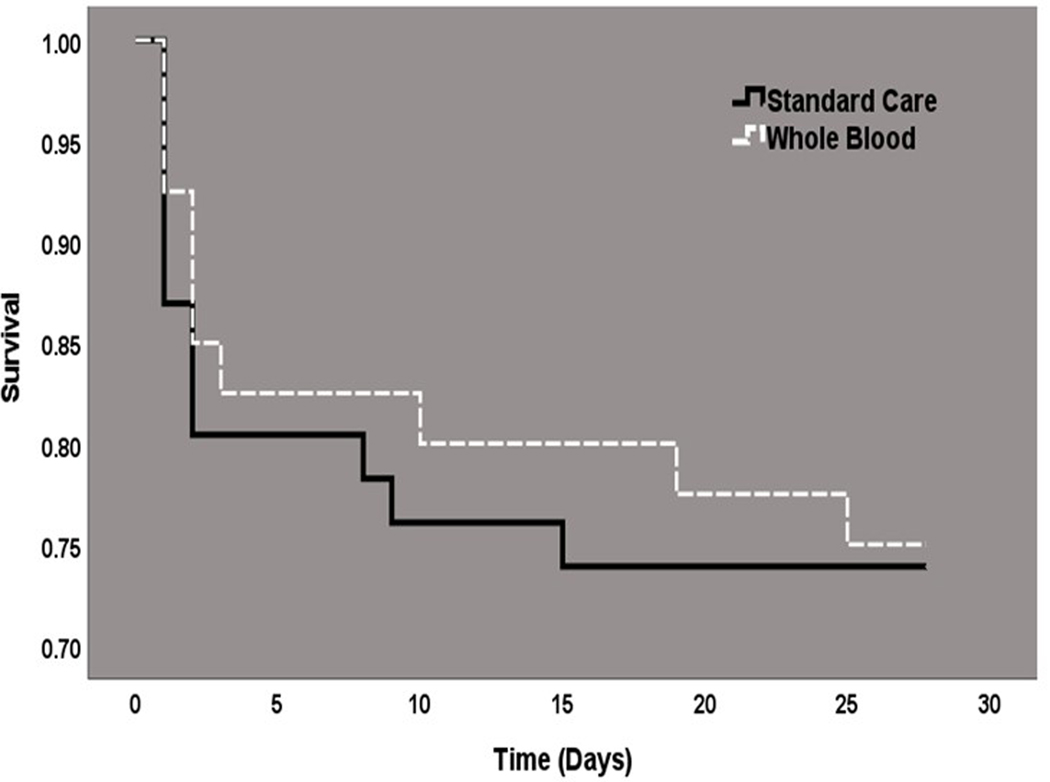
Results: Between November 2018 and October 2020, 86 injured patients were cluster randomized by helicopter base. The trial has halted early at 77% enrollment. Overall, 28-day mortality for the cohort was 26%. Injured patients randomized to prehospital LTOWB (n = 40) relative to standard care (n = 46) were similar in demographics and injury characteristics. Intent-to-treat Kaplan-Meier survival analysis demonstrated no statistical mortality benefit at 28 days (25.0% vs. 26.1%, p = 0.85). Patients randomized to prehospital LTOWB relative to standard care had lower red cell transfusion requirements at 24 hours (p < 0.01) and a lower incidence of abnormal thromboelastographic measurements. No transfusion reactions during the prehospital or in-hospital phase of care were documented.
Conclusion: Prehospital through in-hospital LTOWB resuscitation is safe and may be associated with hemostatic benefits. A large-scale clinical trial is feasible with protocol adjustment and would allow the effects of prehospital LTOWB on survival and other pertinent clinical outcomes to be appropriately characterized.
Level of evidence: Therapeutic/Care Management, Level II.
Trial registration: ClinicalTrials.gov NCT03477006.
Copyright © 2022 American Association for the Surgery of Trauma.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare
Figures
Comment in
-
Prehospital low titer group O whole blood: Difficult to conclude?J Trauma Acute Care Surg. 2022 Nov 1;93(5):e175. doi: 10.1097/TA.0000000000003637. Epub 2022 Jun 14. J Trauma Acute Care Surg. 2022. PMID: 35696354 No abstract available.
-
Prehosptial low titer group O whole blood is feasible and safe: Results of a prospective randomized pilot trial.J Trauma Acute Care Surg. 2022 Nov 1;93(5):e175-e176. doi: 10.1097/TA.0000000000003686. Epub 2022 Jun 14. J Trauma Acute Care Surg. 2022. PMID: 35696382 No abstract available.
References
-
- Harvin JA, Wray CJ, Steward J, Lawless RA, McNutt MK, Love JD, Moore LJ, Wade CE, Cotton BA, Holcomb JB. Control the damage: morbidity and mortality after emergent trauma laparotomy. Am J Surg. 2016;212(1):34–9. - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–82. - PMC - PubMed
-
- Rhee P, Joseph B, Pandit V, Aziz H, Vercruysse G, Kulvatunyou N, Friese RS. Increasing trauma deaths in the United States. Ann Surg. 2014;260(1):13–21. - PubMed
-
- Shackelford SA, Del Junco DJ, Powell-Dunford N, Mazuchowski EL, Howard JT, Kotwal RS, Gurney J, Butler FK Jr., Gross K, Stockinger ZT Association of Prehospital Blood Product Transfusion During Medical Evacuation of Combat Casualties in Afghanistan With Acute and 30-Day Survival. JAMA. 2017;318(16):1581–91. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
