

Stage-Oriented CT Classification and Intermodal Evolution Model in Hepatic Alveolar Echinococcosis
- PMID: 35081647
- PMCID: PMC9133419
- DOI: 10.1055/a-1710-3669
Stage-Oriented CT Classification and Intermodal Evolution Model in Hepatic Alveolar Echinococcosis
Abstract
Background: Alveolar echinococcosis (AE) is one of the most dangerous human parasitoses. The main site of disease manifestation is the liver (about 98 %). The Echinococcus Multilocularis Ulm Classification for Computed Tomography (EMUC-CT), presented in 2016, was the first compilation of CT morphological criteria of hepatic AE. Studies based on EMUC-CT made it possible to draw conclusions about the development of the lesions in the course of disease beyond purely diagnostic typing. Among the most important findings of these precursor studies was that EMUC-CT type IV presented as an initial lesion, whereas EMUC-CT type III lesions were mostly associated with an advanced disease constellation. An intermodal view of image morphological criteria provides further multi-layered indications for lesion evolution.
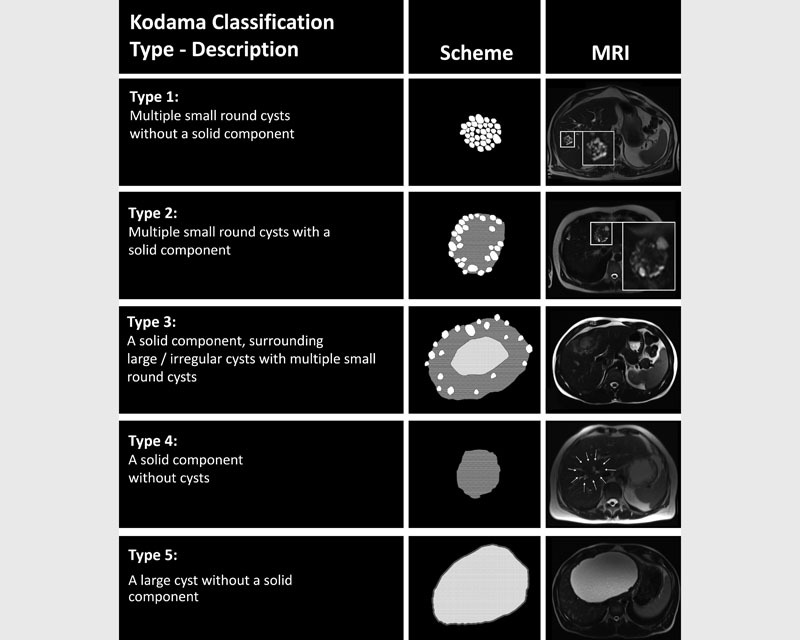
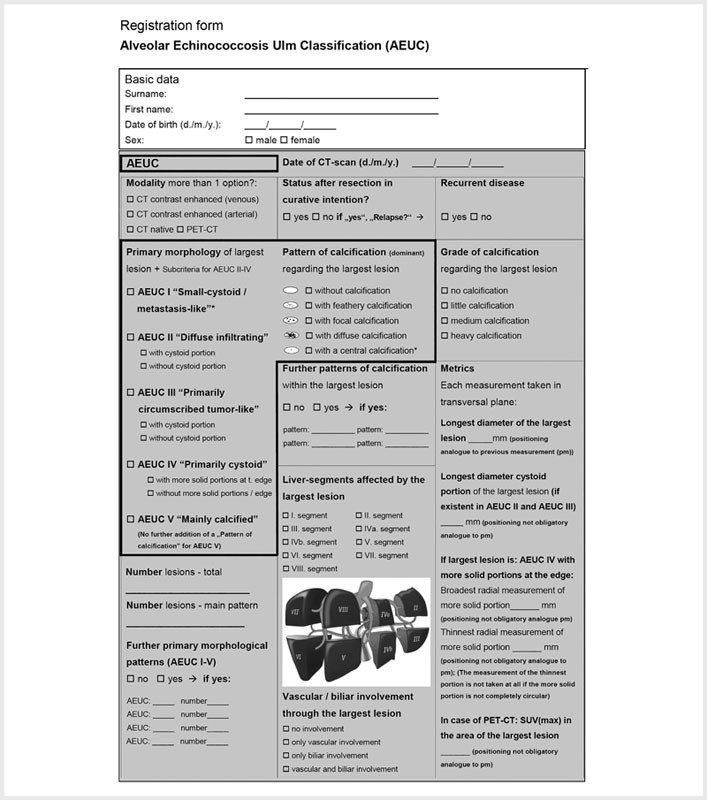
Method: With the "Alveolar Echinococcosis Ulm Classification" (AEUC), a revision of the previous EMUC-CT was carried out with stage-oriented reorganization of the primary morphologies. Furthermore, an intermodal classification scheme for the evolution of hepatic AE lesions based on AEUC, MRI Kodama classification, and aspects of ultrasound could be outlined.
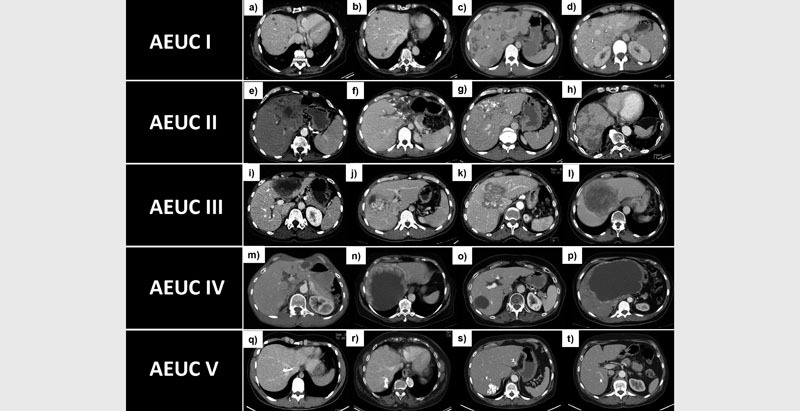
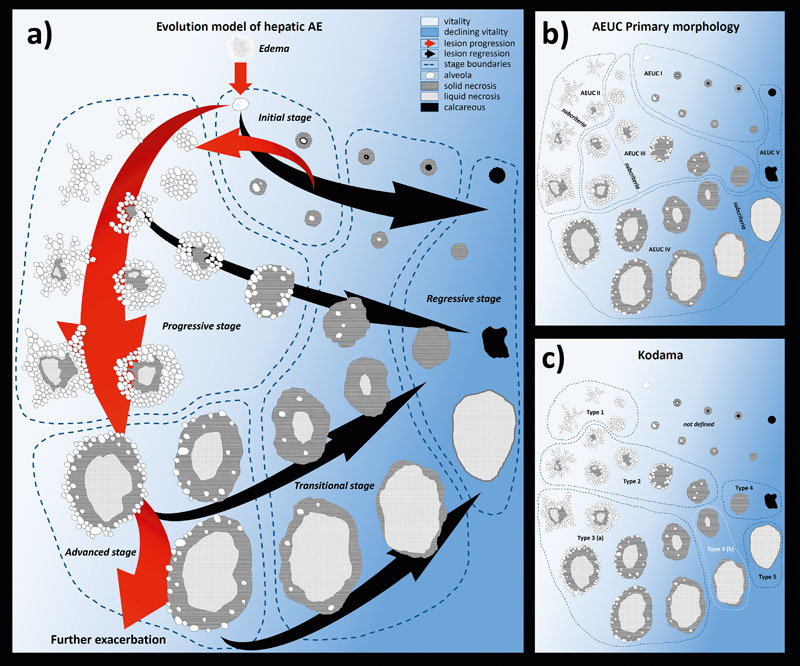
Results: The first stage-oriented CT classification of hepatic AE "AEUC" is based with respect to its lesion characterization on the separate consideration of two classification pillars, the five "primary morphologies", AEUC I-V (AEUC II-IV with subcriteria) and the five "patterns of calcification". In addition, an intermodal classification scheme presents five stages of lesion evolution: "initial stage", "progressive stage", "advanced stage", "transitional stage" and "regressive stage".
Conclusion: The imaging modalities differ with respect to their visualization of lesion criteria. This underlines the need for unimodal classification systems. Staging of an AE lesion can be done more accurately by evaluating different modalities.
Key points: · The AEUC provides a stage-oriented CT classification for hepatic AE.. · Aspects of different modalities allow a more multi-layered view of lesion evolution.. · More accurate staging can be achieved by combining different modalities..
Citation format: · Graeter T, Schmidberger J. Stage-Oriented CT Classification and Intermodal Evolution Model in Hepatic Alveolar Echinococcosis. Fortschr Röntgenstr 2022; 194: 532 - 544.
Die alveoläre Echinokokkose (AE) ist eine der gefährlichsten humanen Parasitosen. Hauptmanifestationsort der Erkrankung ist mit etwa 98 % die Leber. Die 2016 vorgestellte „Echinococcus Multilocularis Ulm Classification for Computed Tomography“ (EMUC-CT) war die erste Zusammenstellung CT-morphologischer Kriterien der hepatischen AE. Studien auf Basis der EMUC-CT ermöglichten es, über die rein diagnostische Typisierung hinaus Rückschlüsse auf die Entwicklung der Läsionen im Krankheitsverlauf zu ziehen. Zu den wichtigsten Erkenntnissen dieser Vorläuferstudien gehörte, dass sich Typ IV der EMUC-CT als Initialläsion präsentierte, während EMUC-CT Typ III-Läsionen meist mit einer fortgeschrittenen Krankheitskonstellation verbunden waren. Eine intermodale Betrachtung bildmorphologischer Kriterien gibt weitere Hinweise für eine Läsionsevolution.Mit der „Alveolar Echinococcosis Ulm Classification“ (AEUC) erfolgte eine Revision der bisherigen EMUC-CT mit einer stadienorientierten Neuordnung der Primärmorphologien. Zudem konnte ein intermodales Klassifikationsschema zur Evolution hepatischer AE-Läsionen anhand der AEUC, der MRT Kodama-Klassifikation und Aspekten des Ultraschalls skizziert werden.Die erste stadienorientierte CT-Klassifikation hepatischer AE „AEUC“ basiert in ihrer Läsionscharakterisierung auf der getrennten Betrachtung zweier Klassifikationssäulen, den 5 „Primärmorphologien“, AEUC I–V (AEUC II–IV mit Subkriterien), und den 5 „Kalzifikationsmustern“. Darüber hinaus präsentiert ein intermodales Klassifikationsschema 5 Stadien der Läsionsevolution: „Initialstadium“, „Progressionsstadium“, „fortgeschrittenes Stadium“, „Übergangsstadium“ und „Regressionsstadium“.Die bildgebenden Modalitäten unterscheiden sich in der Darstellung von Läsionskriterien. Dies unterstreicht die Notwendigkeit unimodaler Klassifikationssysteme. Die Stadienzuordnung einer AE-Läsion kann unter Wertung verschiedener Modalitäten genauer erfolgen. · Die AEUC bietet eine stadienorientierte CT-Klassifikation bei hepatischer AE.. · Aspekte unterschiedlicher Modalitäten ermöglichen eine vielschichtigere Betrachtung der Läsionsevolution.. · Eine genauere Stadienzuordnung kann durch die Kombination verschiedener Modalitäten erreicht werden.. · Graeter T, Schmidberger J. Stage-Oriented CT Classification and Intermodal Evolution Model in Hepatic Alveolar Echinococcosis. Fortschr Röntgenstr 2022; 194: 532 – 544.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commecial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures









References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources