

Uncovering the treatable burden of severe aortic stenosis in the UK
- PMID: 35082136
- PMCID: PMC8739674
- DOI: 10.1136/openhrt-2021-001783
Uncovering the treatable burden of severe aortic stenosis in the UK
Abstract
Objective: To estimate the population prevalence and treatable burden of severe aortic stenosis (AS) in the UK.
Methods: We adapted a contemporary model of the population profile of symptomatic and asymptomatic severe AS in Europe and North America to estimate the number of people aged ≥55 years in the UK who might benefit from surgical aortic valve replacement (SAVR) or transcatheter aortic valve implantation (TAVI).
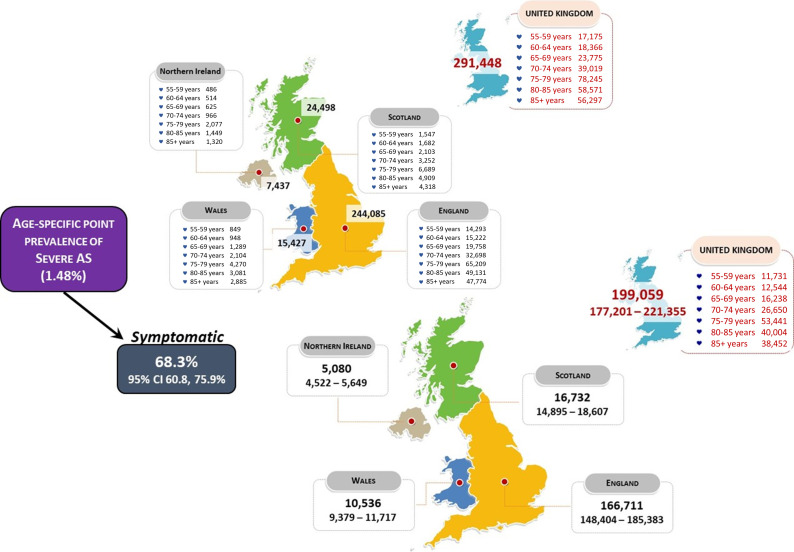
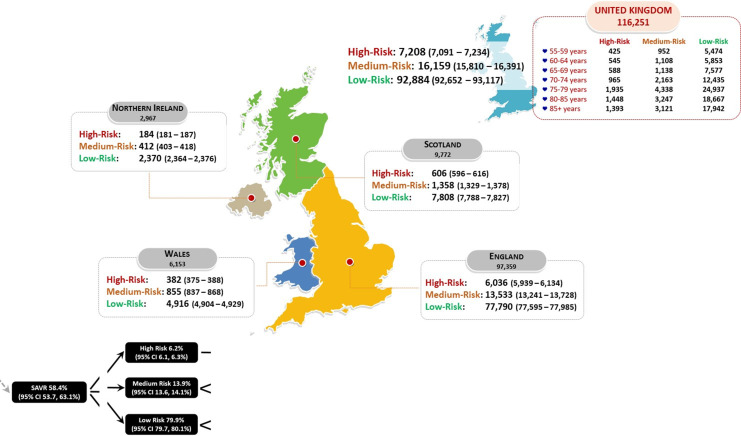
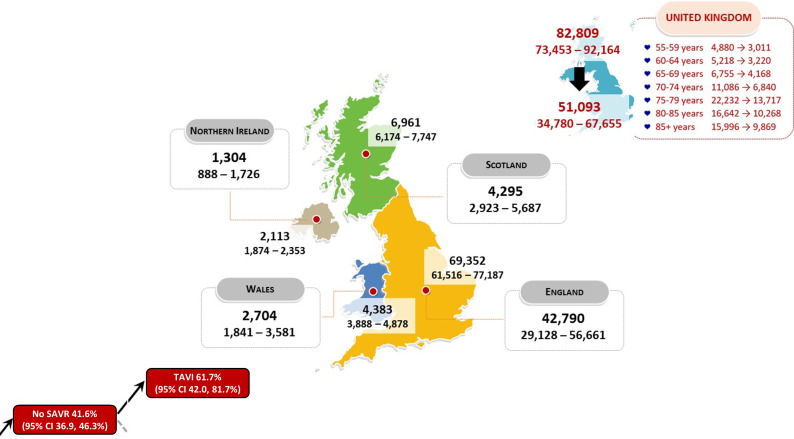
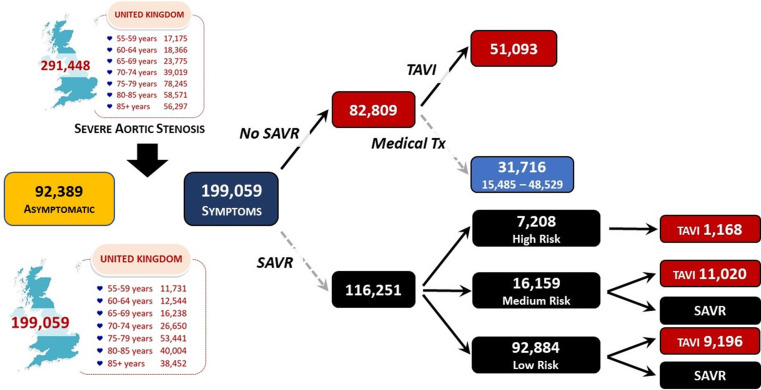
Results: With a point prevalence of 1.48%, we estimate that 291 448 men and women aged ≥55 years in the UK had severe AS in 2019. Of these, 68.3% (199 059, 95% CI 1 77 201 to 221 355 people) would have been symptomatic and, therefore, more readily treated according to their surgical risk profile; the remaining 31.7% of cases (92 389, 95% CI 70 093 to 144 247) being asymptomatic. Based on historical patterns of intervention, 58.4% (116 251, 95% CI 106 895 to 1 25 606) of the 199 059 symptomatic cases would qualify for SAVR, with 7208 (95% CI 7091 to 7234) being assessed as being in a high, preoperative surgical risk category. Among the remaining 41.6% (82 809, 95% CI 73 453 to 92 164) of cases potentially unsuitable for SAVR, an estimated 61.7% (51 093, 95% CI 34 780 to 67 655) might be suitable for TAVI. We estimate that 172 859 out of 291 448 prevalent cases of severe AS (59.3%) will subsequently die within 5 years without proactive management.
Conclusions: These data suggest a high burden of severe AS in the UK requiring surgical or transcatheter intervention that challenges the ongoing capacity of the National Health Service to meet the needs of those affected.
Keywords: aortic valve stenosis; cardiac surgical procedures; transcatheter aortic valve replacement.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: GS: Research grants: Actelion, Bayer, Edwards, GSK, Jensen, Novartis. Consultancies: Edwards, Echo IQ, NEDA Ltd. SS: Research grants: Actelion, Bayer, Edwards, GSK, Jensen, Novartis. NC: Research grants: Boston Scientific, HeartFlow, Beckmann Coulter. Speaker Fees/Consultancy: HeartFlow, Abbott, Edwards. Travel Sponsorship: HeartFlow, Boston Scientific, Biosensors, Medtronic, Edwards. PB: Honoraria: Edwards Lifesciences and Atricure Ltd. DP: Research grants: Actelion, Bayer, Edwards, GSK, Jensen, Novartis. HHG: Consultancies: Wilmington Healthcare, Edwards Lifesciences, Heart Valve Voice.
Figures

References
-
- Beyersdorf F, Praz F, Milojevic M. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J 2021;00:1–72. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials