

Histoplasmosis in African children: clinical features, diagnosis and treatment
- PMID: 35083042
- PMCID: PMC8785273
- DOI: 10.1177/20499361211068592
Histoplasmosis in African children: clinical features, diagnosis and treatment
Abstract
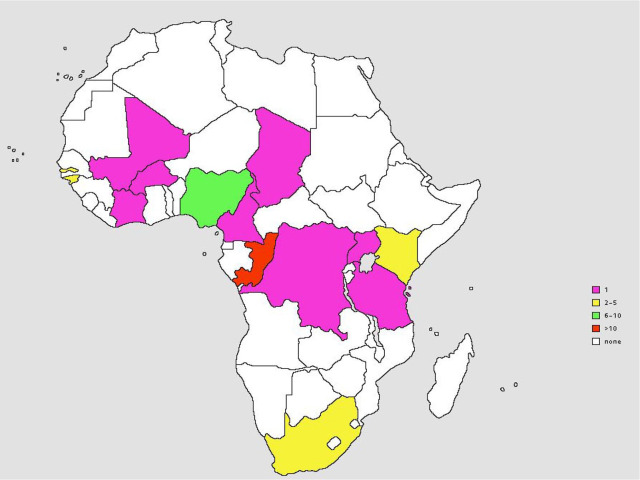
Most of the reviews on histoplasmosis documented in literature have been in the adult population. Very few studies highlight the peculiarities associated with histoplasmosis in Africa especially in the pediatric population. This review addresses the above concerns with clinical summaries and diagnosis of some case reports of histoplasmosis in African children. We highlighted 44 case reports of histoplasmosis in African children (1950-2021) distributed across Western Africa (38.6%, n = 17), Eastern Africa (9.1%, n = 4), Southern Africa (9.1%, n = 4), and Central Africa (43.2%, n = 19). No case report was found from Northern Africa. The age range was 1-17 years, with a mean of 9.2. Of the 44 case reports, 8 cases (18.2%, 8/44) were caused by Histoplasma capsulatum var capsulatum, 33 cases (75%, 33/44) were caused by Histoplasma capsulatum var duboisii, and specie identification was not found in 3 cases. Only three (6.8%) cases were HIV positive; 56.8% (25/44) were disseminated histoplasmosis, pulmonary histoplasmosis accounted for just one case (2.3%, 1/44). Extrapulmonary presentation included skin lesions (ulcers, fistulas, nodules, patches, pigmentations, papules, and abscesses), bone lesions, osteoarthritis, and fractures. The commonest sites affected were skin (n = 29, 65.9%), bones (n = 20, 45.5%), and lymph nodes (n = 15, 34.1%). Histopathology was the commonest diagnostic method (n = 33, 75%). Amphotericin B was first-line therapy in 45.5% of the cases (n = 20) followed by ketoconazole (20.5%, n = 9); 27 cases (61.4%) had favorable outcomes, 8 cases (18.2%) had fatal outcomes, while in 9 cases, the outcome was not revealed. This review revealed several cases of histoplasmosis misdiagnosed as other conditions including tuberculosis (n = 3, 6.8%), pneumonia (n = 1, 2.3%), cancers (n = 4, 9.1%), nephritic syndrome (n = 1, 2.3%), leishmaniasis (n = 1, 2.3%), and hyperreactive malarial splenomegaly syndrome (n = 1, 2.3%). In addition, histoplasmosis was not considered in some case reports even when symptoms were suggestive. Diagnosis of histoplasmosis was made at autopsy with postmortem findings suggestive of histoplasmosis (n = 3, 6.8%). This report highlights the need for a paradigm shift on the part of pediatricians in Africa. They need to look beyond clinical conditions considered common in our environment for this age group and evaluate for other diseases including histoplasmosis.
Keywords: Africa; Histoplasma duboisii; children; disseminated histoplasmosis; histoplasmosis; tuberculosis.
© The Author(s), 2022.
Conflict of interest statement
Conflict of interest statement: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
