Evidence for shared genetic risk factors between lymphangioleiomyomatosis and pulmonary function
- PMID: 35083324
- PMCID: PMC8784893
- DOI: 10.1183/23120541.00375-2021
Evidence for shared genetic risk factors between lymphangioleiomyomatosis and pulmonary function
Abstract
Introduction: Lymphangioleiomyomatosis (LAM) is a rare low-grade metastasising disease characterised by cystic lung destruction. The genetic basis of LAM remains incompletely determined, and the disease cell-of-origin is uncertain. We analysed the possibility of a shared genetic basis between LAM and cancer, and LAM and pulmonary function.
Methods: The results of genome-wide association studies of LAM, 17 cancer types and spirometry measures (forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC ratio and peak expiratory flow (PEF)) were analysed for genetic correlations, shared genetic variants and causality. Genomic and transcriptomic data were examined, and immunodetection assays were performed to evaluate pleiotropic genes.
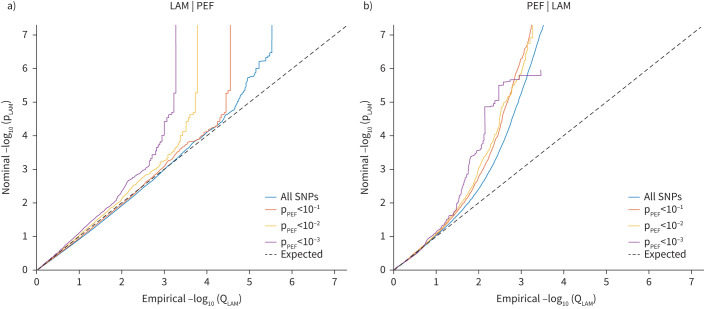
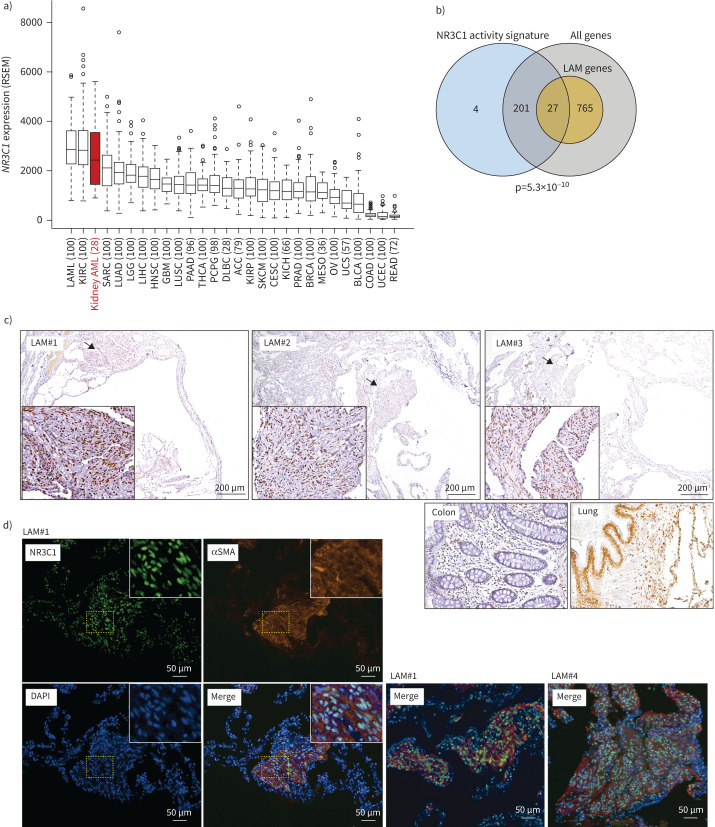
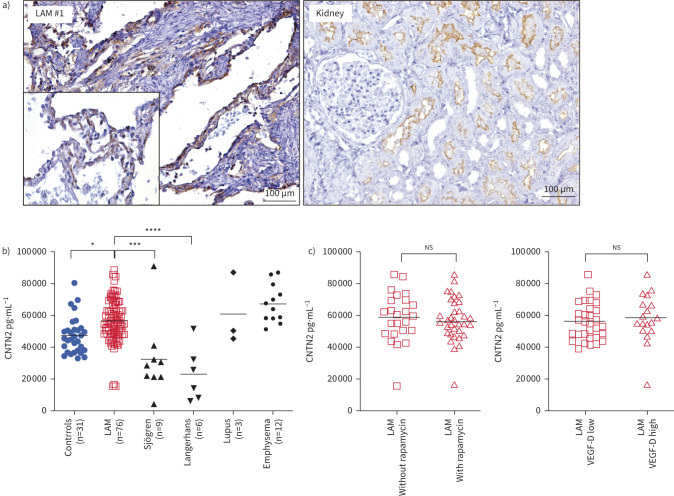
Results: There were no significant overall genetic correlations between LAM and cancer, but LAM correlated negatively with FVC and PEF, and a trend in the same direction was observed for FEV1. 22 shared genetic variants were uncovered between LAM and pulmonary function, while seven shared variants were identified between LAM and cancer. The LAM-pulmonary function shared genetics identified four pleiotropic genes previously recognised in LAM single-cell transcriptomes: ADAM12, BNC2, NR2F2 and SP5. We had previously associated NR2F2 variants with LAM, and we identified its functional partner NR3C1 as another pleotropic factor. NR3C1 expression was confirmed in LAM lung lesions. Another candidate pleiotropic factor, CNTN2, was found more abundant in plasma of LAM patients than that of healthy women.
Conclusions: This study suggests the existence of a common genetic aetiology between LAM and pulmonary function.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: X. Farré has nothing to disclose. Conflict of interest: R. Espín has nothing to disclose. Conflict of interest: A. Baiges has nothing to disclose. Conflict of interest: E. Blommaert has nothing to disclose. Conflict of interest: W. Kim has nothing to disclose. Conflict of interest: K. Giannikou has nothing to disclose. Conflict of interest: C. Herranz has nothing to disclose. Conflict of interest: A. Román has nothing to disclose. Conflict of interest: B. Sáez has nothing to disclose. Conflict of interest: Á. Casanova has nothing to disclose. Conflict of interest: J. Ancochea has nothing to disclose. Conflict of interest: C. Valenzuela has nothing to disclose. Conflict of interest: P. Ussetti has nothing to disclose. Conflict of interest: R. Laporta has nothing to disclose. Conflict of interest: J.A. Rodríguez-Portal has nothing to disclose. Conflict of interest: C.H.M. van Moorsel has nothing to disclose. Conflict of interest: J.J. van der Vis has nothing to disclose. Conflict of interest: M.J.R. Quanjel has nothing to disclose. Conflict of interest: M. Tena-Garitaonaindia has nothing to disclose. Conflict of interest: F. Sánchez de Medina has nothing to disclose. Conflict of interest: F. Mateo has nothing to disclose. Conflict of interest: M. Molina-Molina has nothing to disclose. Conflict of interest: S. Won has nothing to disclose. Conflict of interest: D.J. Kwiatkowski has nothing to disclose. Conflict of interest: R. de Cid has nothing to disclose. Conflict of interest: M.A. Pujana has nothing to disclose. Support statement: This research was supported by Asociación Española de LAM; The LAM Foundation Seed Grant 2019; Carlos III Institute of Health grants PI18/01029, PI21/01306 and ICI19/00047 (co-funded by European Regional Development Fund (ERDF), “A way to build Europe”); Ministry of Economy and Competitivity grant SAF2017-88457-R; the Generalitat de Catalunya SGR 2017-449 and 2017-529; PERIS PFI-Salut SLT017-20-000076; and the CERCA Program to IDIBELL and Institut Germans Trias i Pujol. X. Farré is supported by the VEIS project (001-P-001647, ERDF Operational Programme of Catalonia 2014–2020; co-funded by ERDF, “A way to build Europe”). Funding information for this article has been deposited with the Crossref Funder Registry.
Figures