

Association Between Hemagglutination Inhibition Antibody Titers and Protection Against Reverse-Transcription Polymerase Chain Reaction-Confirmed Influenza Illness in Children 6-35 Months of Age: Statistical Evaluation of a Correlate of Protection
- PMID: 35083365
- PMCID: PMC8786493
- DOI: 10.1093/ofid/ofab477
Association Between Hemagglutination Inhibition Antibody Titers and Protection Against Reverse-Transcription Polymerase Chain Reaction-Confirmed Influenza Illness in Children 6-35 Months of Age: Statistical Evaluation of a Correlate of Protection
Abstract
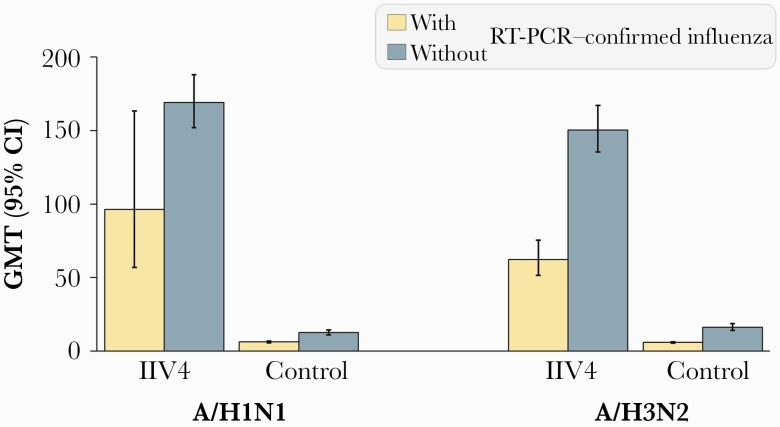
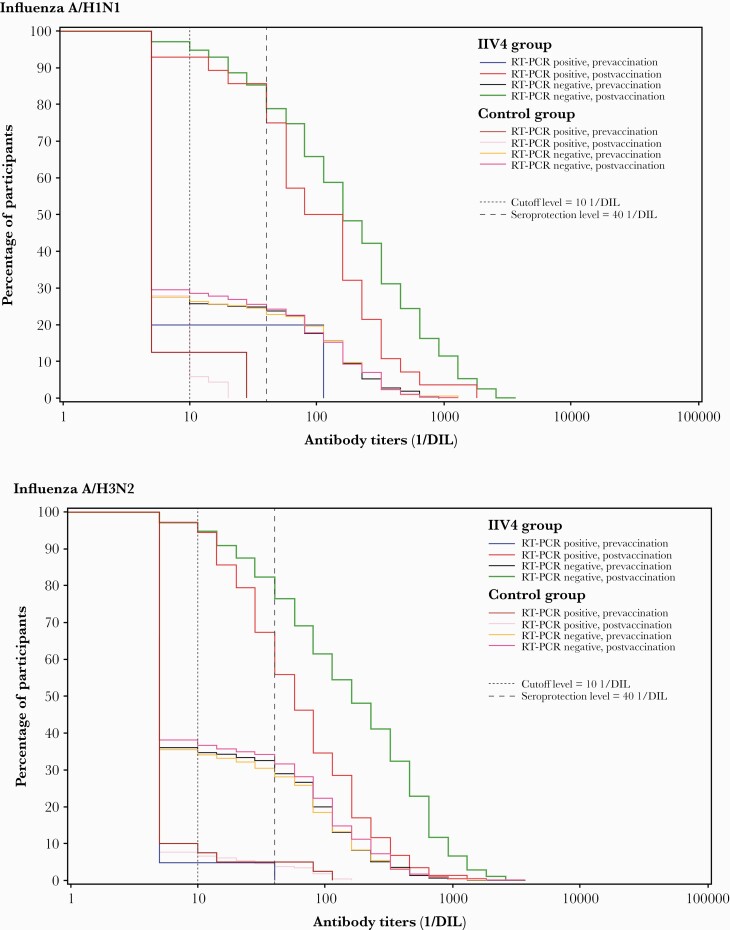
Background: Data from a randomized controlled efficacy trial of an inactivated quadrivalent influenza vaccine in children 6-35 months of age were used to determine whether hemagglutination inhibition (HI) antibody titer against A/H1N1 and A/H3N2 is a statistical correlate of protection (CoP) for the risk of reverse-transcription polymerase chain reaction (RT-PCR)-confirmed influenza associated with the corresponding strain.
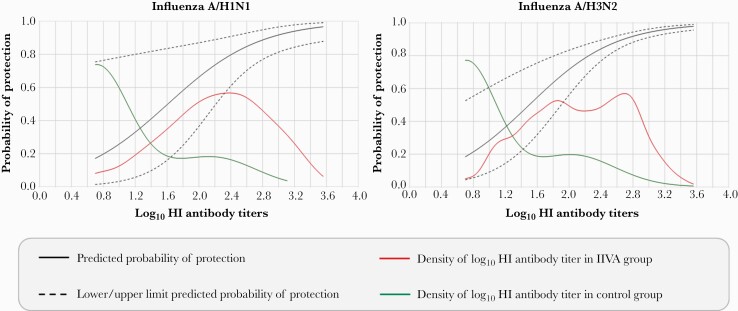
Methods: The Prentice criteria were used to statistically validate strain-specific HI antibody titer as a CoP. The probability of protection was identified using the Dunning model corresponding to a prespecified probability of protection at an individual level. The group-level protective threshold was identified using the Siber approach, leading to unbiased predicted vaccine efficacy (VE). A case-cohort subsample was used for this exploratory analysis.
Results: Prentice criteria confirmed that HI titer is a statistical CoP for RT-PCR-confirmed influenza. The Dunning model predicted a probability of protection of 49.7% against A/H1N1 influenza and 54.7% against A/H3N2 influenza at an HI antibody titer of 1:40 for the corresponding strain. Higher titers of 1:320 were associated with >80% probability of protection. The Siber method predicted VE of 61.0% at a threshold of 1:80 for A/H1N1 and 46.6% at 1:113 for A/H3N2.
Conclusions: The study validated HI antibody titer as a statistical CoP, by demonstrating that HI titer is correlated with clinical protection against RT-PCR-confirmed influenza associated with the corresponding influenza strain and is predictive of VE in children 6-35 months of age.
Clinical trials registration: NCT01439360.
Keywords: HI antibodies; children; correlate of protection; influenza.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Hurwitz ES, Haber M, Chang A, et al. . Studies of the 1996-1997 inactivated influenza vaccine among children attending day care: immunologic response, protection against infection, and clinical effectiveness. J Infect Dis 2000; 182:1218–21. - PubMed
-
- Vesikari T, Knuf M, Wutzler P, et al. . Oil-in-water emulsion adjuvant with influenza vaccine in young children. N Engl J Med 2011; 365:1406–16. - PubMed
-
- Hoberman A, Greenberg DP, Paradise JL, et al. . Effectiveness of inactivated influenza vaccine in preventing acute otitis media in young children: a randomized controlled trial. JAMA 2003; 290:1608–16. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
