

Association of Genetic Ancestry With the Molecular Subtypes and Prognosis of Childhood Acute Lymphoblastic Leukemia
- PMID: 35084434
- PMCID: PMC8796058
- DOI: 10.1001/jamaoncol.2021.6826
Association of Genetic Ancestry With the Molecular Subtypes and Prognosis of Childhood Acute Lymphoblastic Leukemia
Erratum in
-
Error in Figure.JAMA Oncol. 2022 Mar 1;8(3):484. doi: 10.1001/jamaoncol.2022.0283. JAMA Oncol. 2022. PMID: 35297978 Free PMC article. No abstract available.
Abstract
Importance: Racial and ethnic disparities persist in the incidence and treatment outcomes of childhood acute lymphoblastic leukemia (ALL). However, there is a paucity of data describing the genetic basis of these disparities, especially in association with modern ALL molecular taxonomy and in the context of contemporary treatment regimens.
Objective: To evaluate the association of genetic ancestry with childhood ALL molecular subtypes and outcomes of modern ALL therapy.
Design, setting, and participants: This multinational, multicenter genetic association study was conducted from March 1, 2000, to November 20, 2020, among 2428 children and adolescents with ALL enrolled in frontline trials from the United States, South East Asia (Singapore and Malaysia), and Latin America (Guatemala), representing diverse populations of European, African, Native American, East Asian, and South Asian descent. Statistical analysis was conducted from February 3, 2020, to April 19, 2021.
Main outcomes and measures: Molecular subtypes of ALL and genetic ancestry were comprehensively characterized by performing RNA sequencing. Associations of genetic ancestries with ALL molecular subtypes and treatment outcomes were then evaluated.
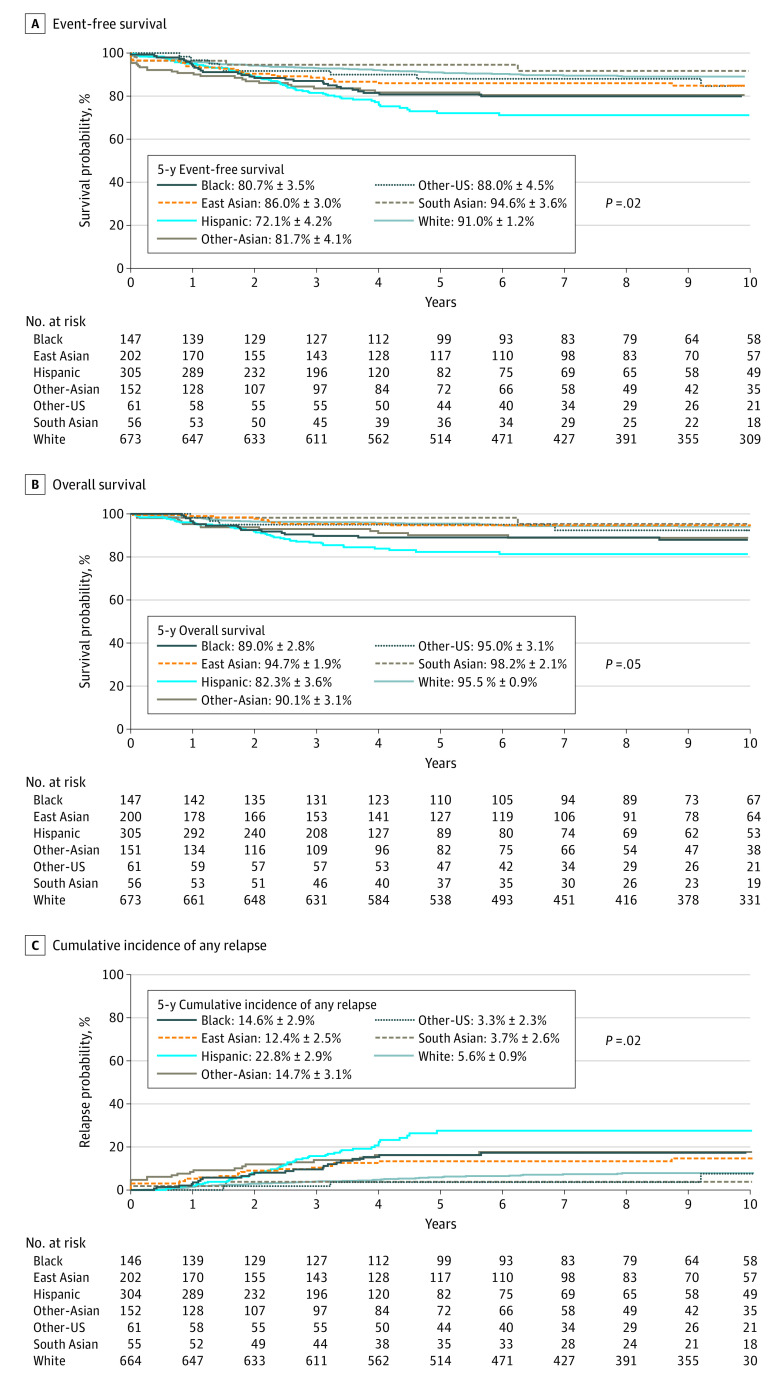
Results: Among the participants in the study, 1340 of 2318 (57.8%) were male, and the mean (SD) age was 7.8 (5.3) years. Of 21 ALL subtypes identified, 8 were associated with ancestry. East Asian ancestry was positively associated with the frequency of somatic DUX4 (odds ratio [OR], 1.30 [95% CI, 1.16-1.45]; P < .001) and ZNF384 (OR, 1.40 [95% CI, 1.18-1.66]; P < .001) gene rearrangements and negatively associated with BCR-ABL1-like ALL (OR, 0.79 [95% CI, 0.66-0.92]; P = .002) and T-cell ALL (OR, 0.80 [95% CI, 0.71-0.90]; P < .001). By contrast, occurrence of CRLF2 rearrangements was associated with Native American ancestry (OR, 1.48 [95% CI, 1.29-1.69]; P < .001). When the percentage of Native American ancestry increased, ETV6-RUNX1 fusion became less frequent (OR, 0.80 [95% CI, 0.70-0.91]; P < .001), with the opposite trend observed for ETV6-RUNX1-like ALL. There was a marked preponderance of T-cell ALL in children of African descent compared with those with a high percentage of Native American ancestry (African: OR, 1.22 [95% CI, 1.07-1.37]; P = .003; Native American: OR, 0.53 [95% CI, 0.40-0.67]; P < .001). African ancestry was also positively associated with the prevalence of TCF3-PBX1 (OR, 1.49 [95% CI, 1.25-1.76]; P < .001) and negatively associated with DUX4 rearrangements (OR, 0.70 [95% CI, 0.48-0.93]; P = .01) and hyperdiploidy (OR, 0.77 [95% CI, 0.68-0.86]; P < .001). African and Native American ancestries as continuous variables were both associated with poorer event-free survival (for every 25% increase in ancestry: hazard ratio [HR], 1.2; 95% CI, 1.1-1.4; P = .001 for African ancestry; HR, 1.3; 95% CI, 1.0-1.6; P = .04 for Native American ancestry) and overall survival (for every 25% increase in ancestry: HR, 1.2; 95% CI, 1.1-1.5; P = .01 for African ancestry; HR, 1.4; 95% CI, 1.0-1.8; P = .03 for Native American ancestry). Even after adjusting for biological subtypes and clinical features, Native American and African ancestries remained associated with poor prognosis.
Conclusions and relevance: This study suggests that ALL molecular subtypes and prognosis are associated with genetic ancestry, potentially pointing to a genetic basis for some of the racial and ethnic disparities in ALL. Therefore, molecular subtype-driven treatment individualization is needed to help address racial and ethnic gaps in outcomes.
Conflict of interest statement
Figures
Comment in
-
Genetic Ancestry and Childhood Acute Lymphoblastic Leukemia Subtypes and Outcomes in the Genomic Era.JAMA Oncol. 2022 Mar 1;8(3):342-343. doi: 10.1001/jamaoncol.2021.6785. JAMA Oncol. 2022. PMID: 35084428 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
