

Effect of sustained high buprenorphine plasma concentrations on fentanyl-induced respiratory depression: A placebo-controlled crossover study in healthy volunteers and opioid-tolerant patients
- PMID: 35085249
- PMCID: PMC8794186
- DOI: 10.1371/journal.pone.0256752
Effect of sustained high buprenorphine plasma concentrations on fentanyl-induced respiratory depression: A placebo-controlled crossover study in healthy volunteers and opioid-tolerant patients
Abstract
Background: Opioid-induced respiratory depression driven by ligand binding to mu-opioid receptors is a leading cause of opioid-related fatalities. Buprenorphine, a partial agonist, binds with high affinity to mu-opioid receptors but displays partial respiratory depression effects. The authors examined whether sustained buprenorphine plasma concentrations similar to those achieved with some extended-release injections used to treat opioid use disorder could reduce the frequency and magnitude of fentanyl-induced respiratory depression.
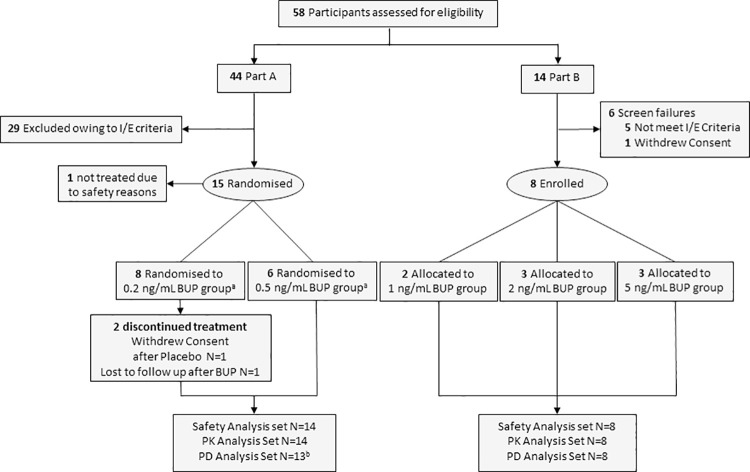
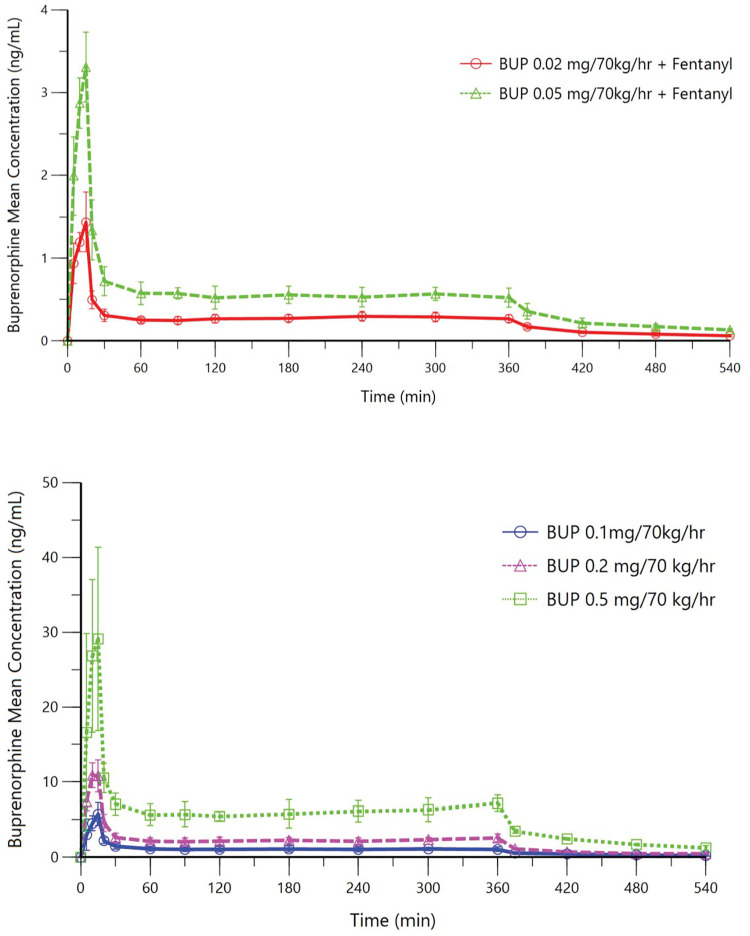
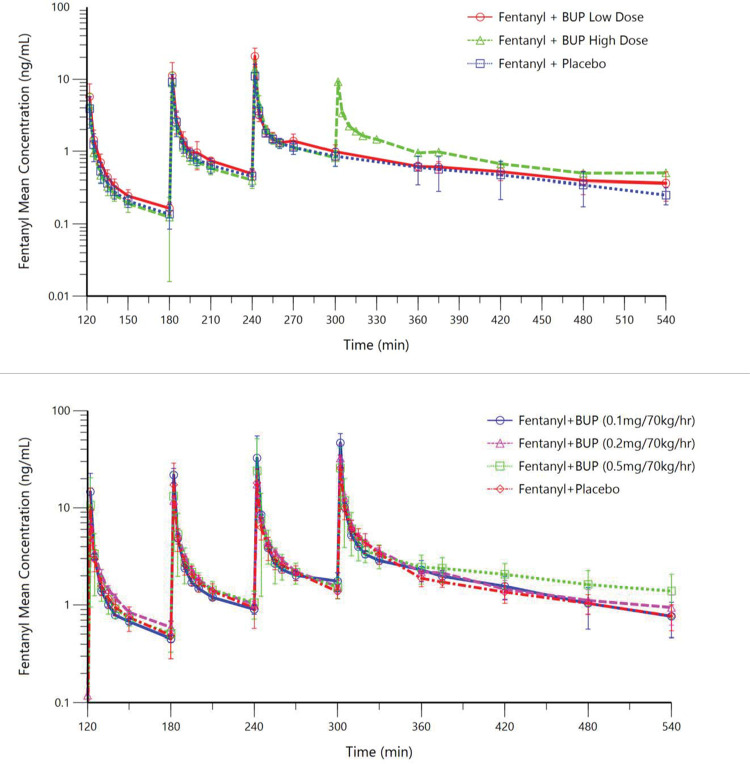
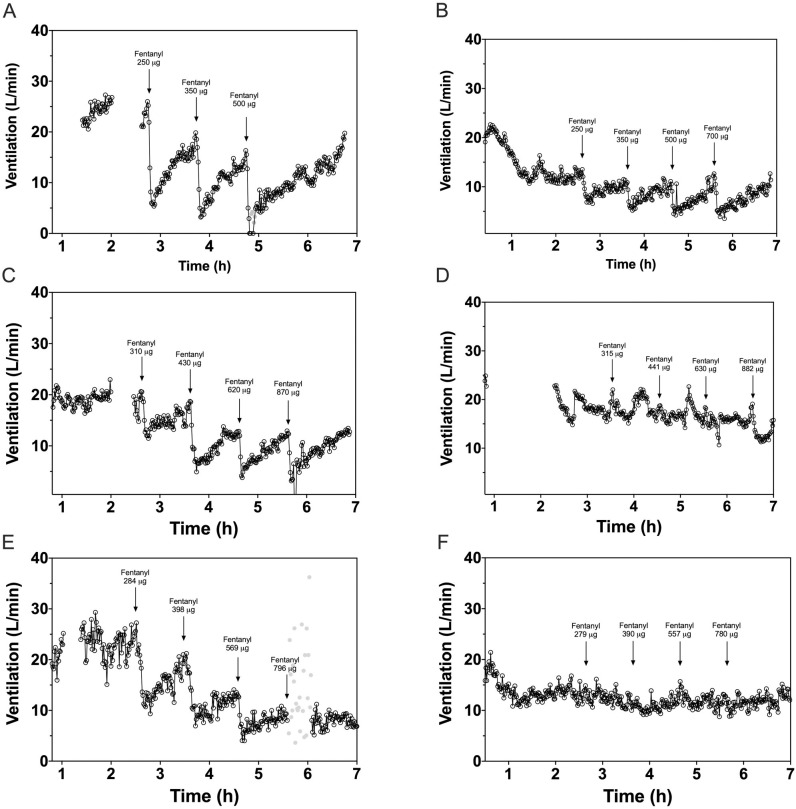
Methods: In this two-period crossover, single-centre study, 14 healthy volunteers (single-blind, randomized) and eight opioid-tolerant patients taking daily opioid doses ≥90 mg oral morphine equivalents (open-label) received continuous intravenous buprenorphine or placebo for 360 minutes, targeting buprenorphine plasma concentrations of 0.2 or 0.5 ng/mL in healthy volunteers and 1.0, 2.0 or 5.0 ng/mL in opioid-tolerant patients. Upon reaching target concentrations, participants received up to four escalating intravenous doses of fentanyl. The primary endpoint was change in isohypercapnic minute ventilation (VE). Additionally, occurrence of apnea was recorded.
Results: Fentanyl-induced changes in VE were smaller at higher buprenorphine plasma concentrations. In healthy volunteers, at target buprenorphine concentration of 0.5 ng/mL, the first and second fentanyl boluses reduced VE by [LSmean (95% CI)] 26% (13-40%) and 47% (37-59%) compared to 51% (38-64%) and 79% (69-89%) during placebo infusion (p = 0.001 and < .001, respectively). Discontinuations for apnea limited treatment comparisons beyond the second fentanyl injection. In opioid-tolerant patients, fentanyl reduced VE up to 49% (21-76%) during buprenorphine infusion (all concentration groups combined) versus up to 100% (68-132%) during placebo infusion (p = 0.006). In opioid-tolerant patients, the risk of experiencing apnea requiring verbal stimulation following fentanyl boluses was lower with buprenorphine than with placebo (odds ratio: 0.07; 95% CI: 0.0 to 0.3; p = 0.001).
Interpretation: Results from this proof-of-principle study provide the first clinical evidence that high sustained plasma concentrations of buprenorphine may protect against respiratory depression induced by potent opioids like fentanyl.
Conflict of interest statement
The authors have read the journal’s policy and have the following competing interests: RD, FG, SS, AH, and CL are paid employees of Indivior Inc. This does not alter our adherence to PLOS ONE policies on sharing data and materials. There are no patents, products in development or marketed products associated with this research to declare.
Figures
References
-
- United Nations Office on Drugs and Crime. World Drug Report 2020, (United Nations publication, Sales No. E.20.XI.6).
-
- Centers for Disease Control and Prevention. 2019 Annual Surveillance Report of Drug-Related Risks and Outcomes—United States Surveillance Special Report. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Published November 1, 2019. https://www.cdc.gov/drugoverdose/pdf/pubs/2019-cdc-drug-surveillance-rep.... Accessed August 25, 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
