

Race- and Gender-Based Differences in Cardiac Structure and Function and Risk of Heart Failure
- PMID: 35086658
- PMCID: PMC8849570
- DOI: 10.1016/j.jacc.2021.11.024
Race- and Gender-Based Differences in Cardiac Structure and Function and Risk of Heart Failure
Abstract
Background: Although heart failure (HF) risk and cardiac structure/function reportedly differ according to race and gender, limited data exist in late life when risk of HF is highest.
Objectives: The goal of this study was to evaluate race/gender-based differences in HF risk factors, cardiac structure/function, and incident HF in late life.
Methods: This analysis included 5,149 HF-free participants from ARIC (Atherosclerosis Risk In Communities), a prospective epidemiologic cohort study, who attended visit 5 (2011-2013) and underwent echocardiography. Participants were subsequently followed up for a median 5.5 years for incident HF/death.
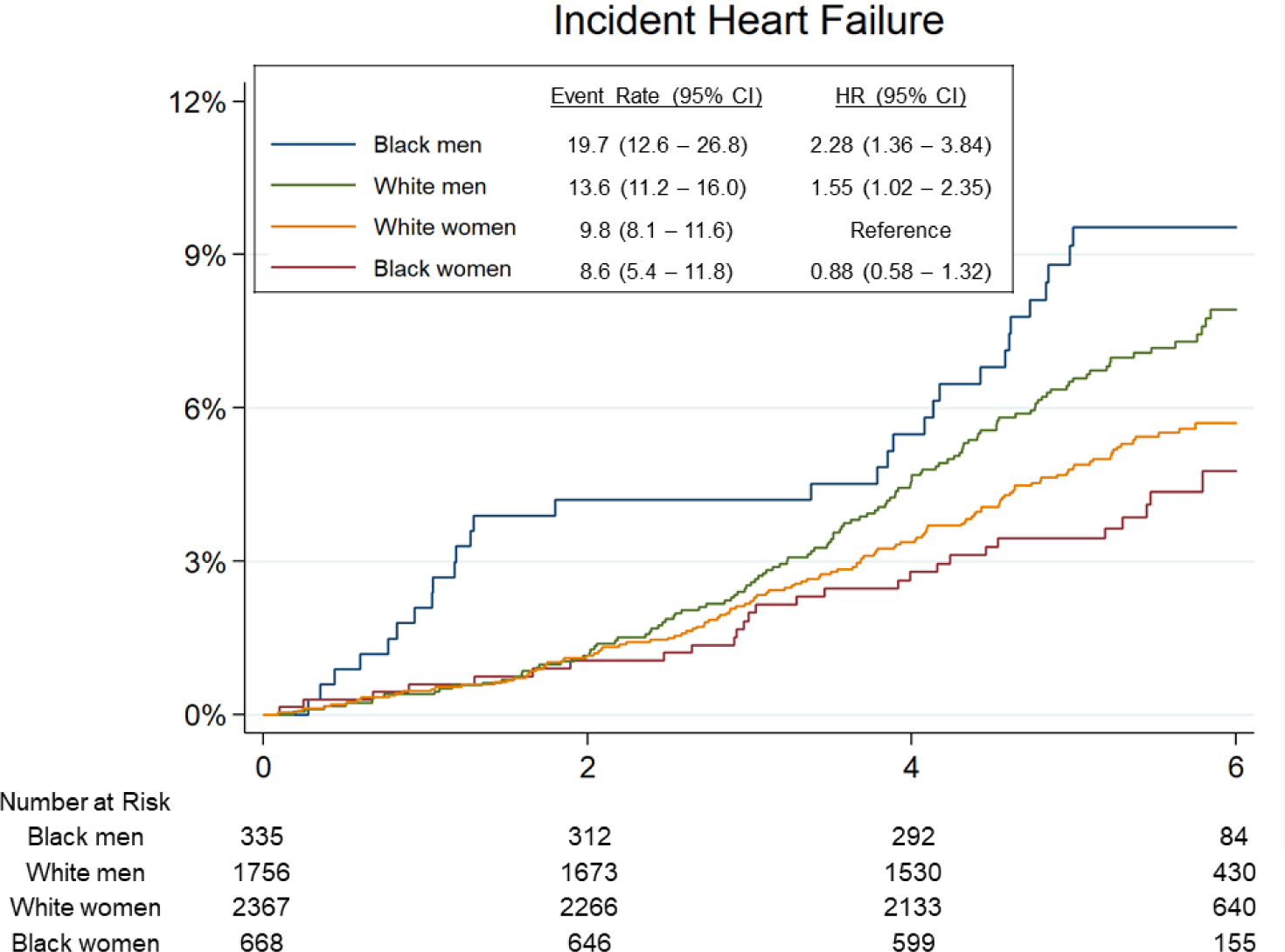
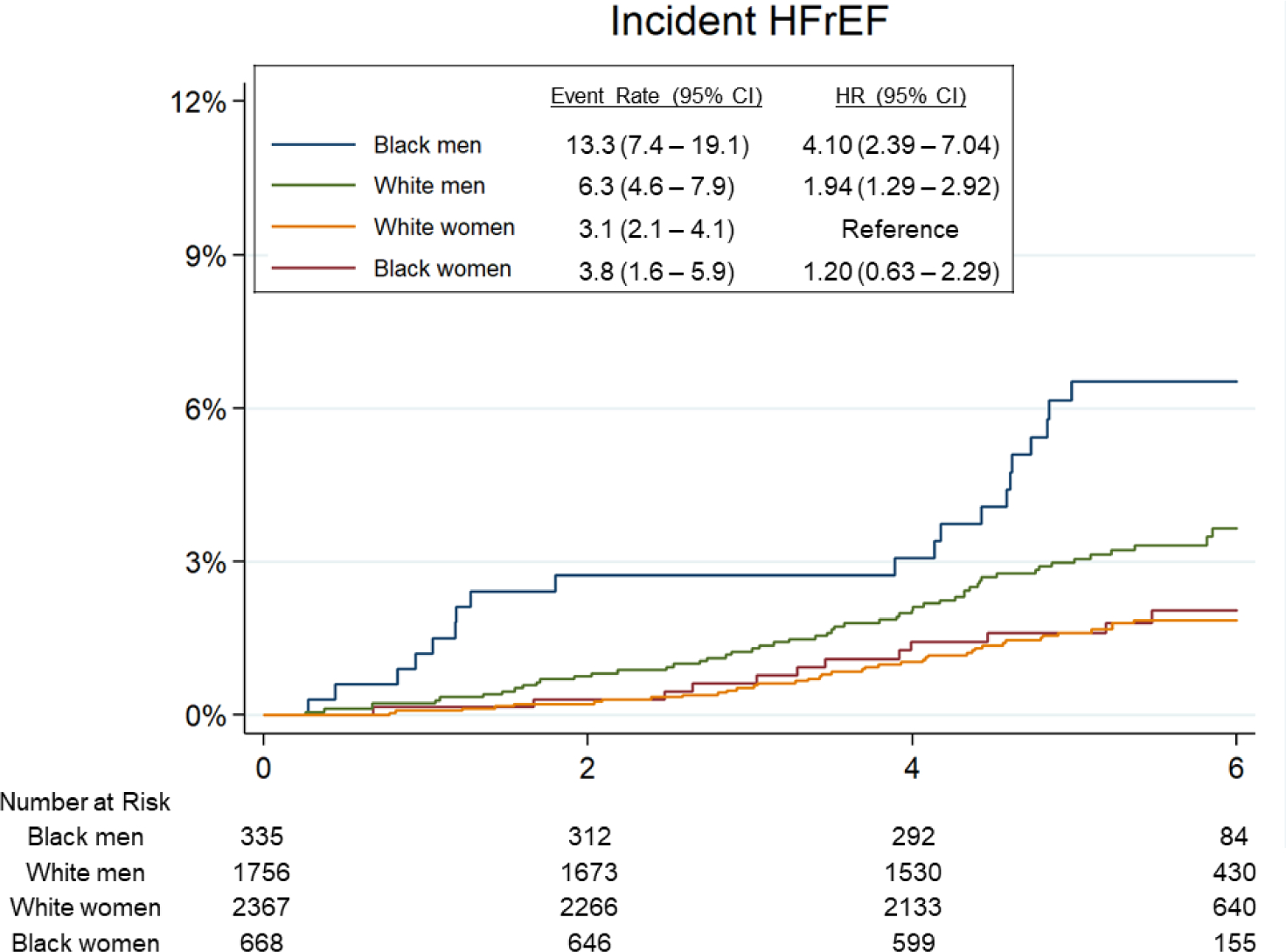
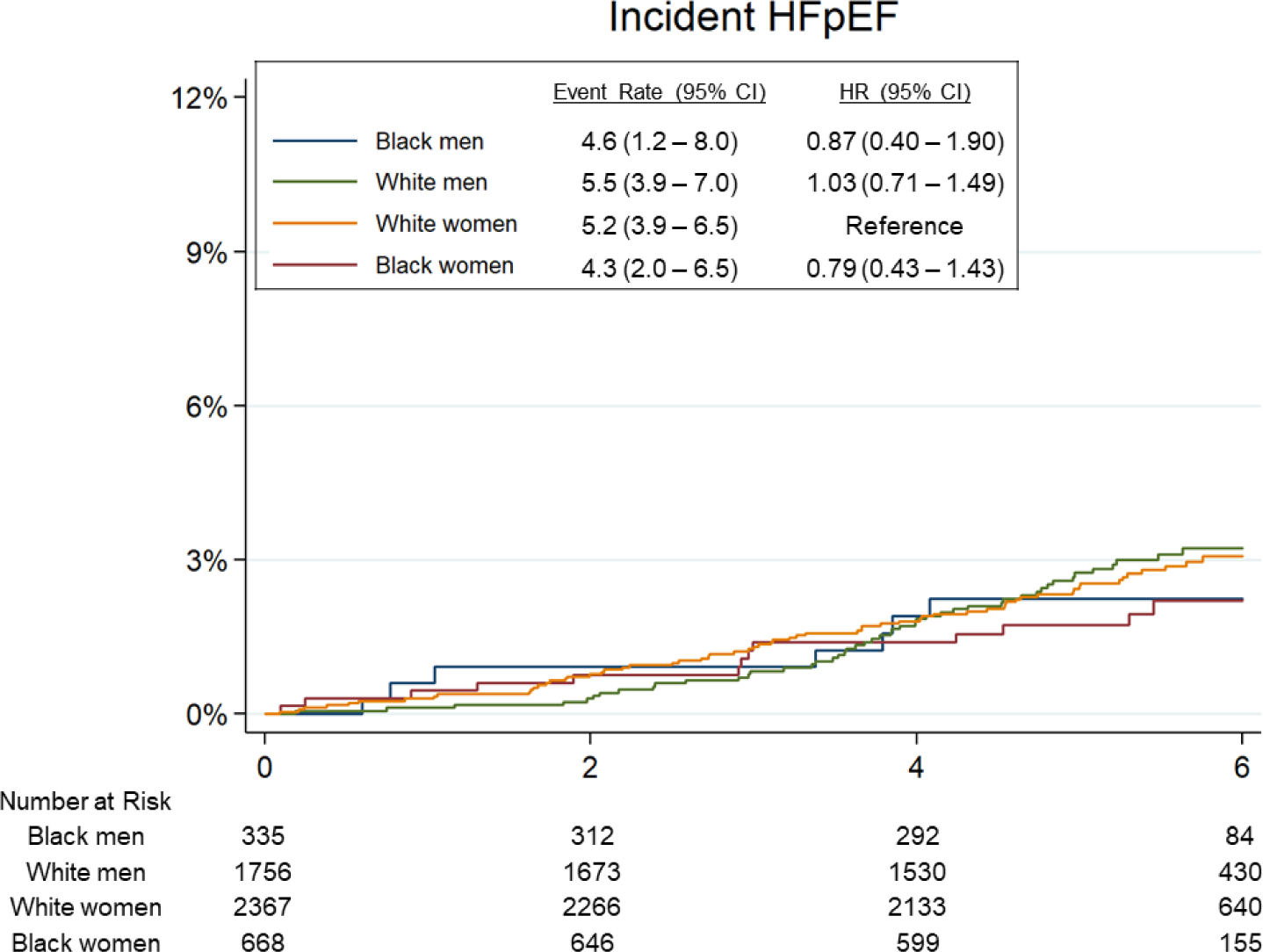
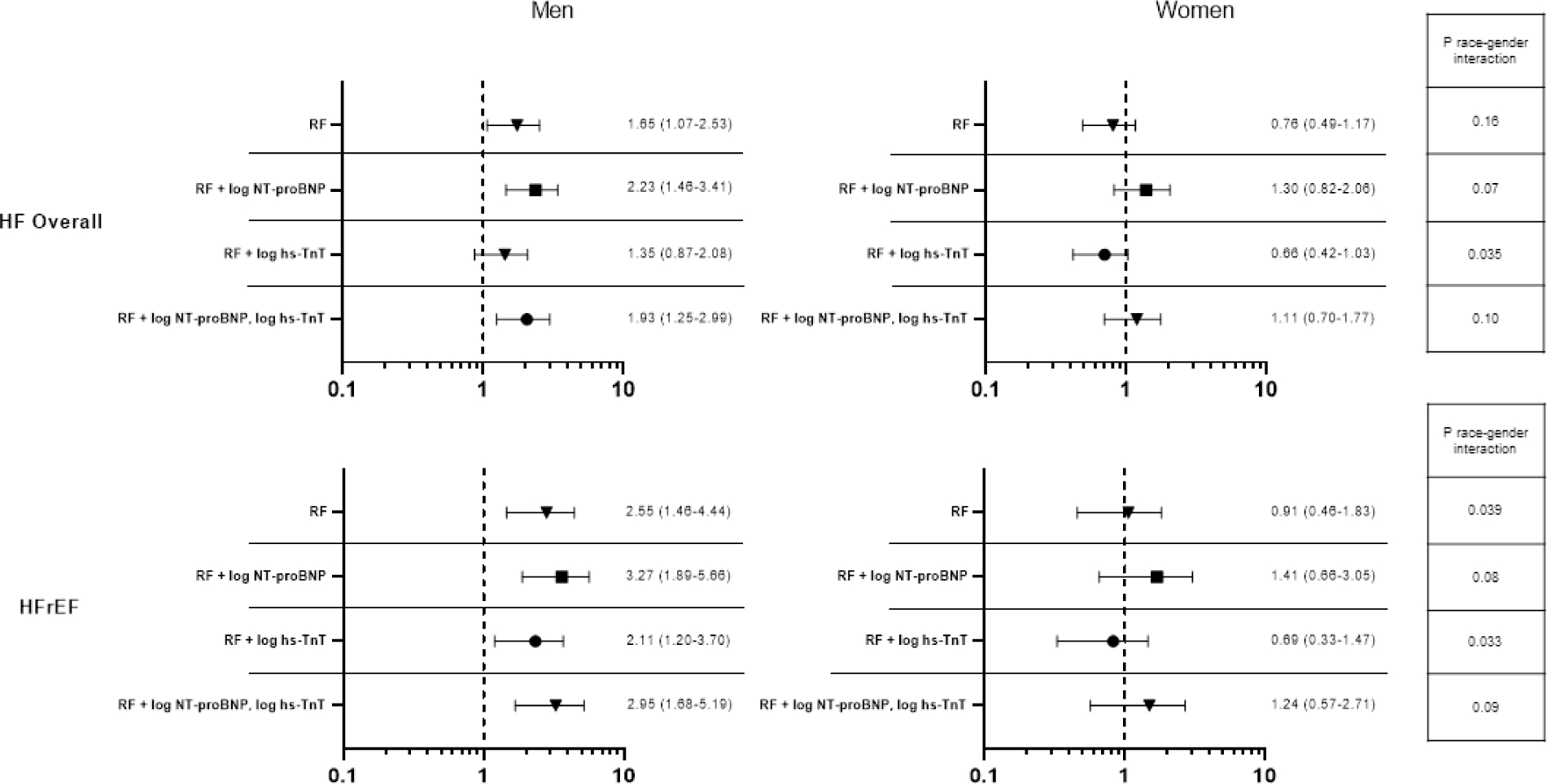
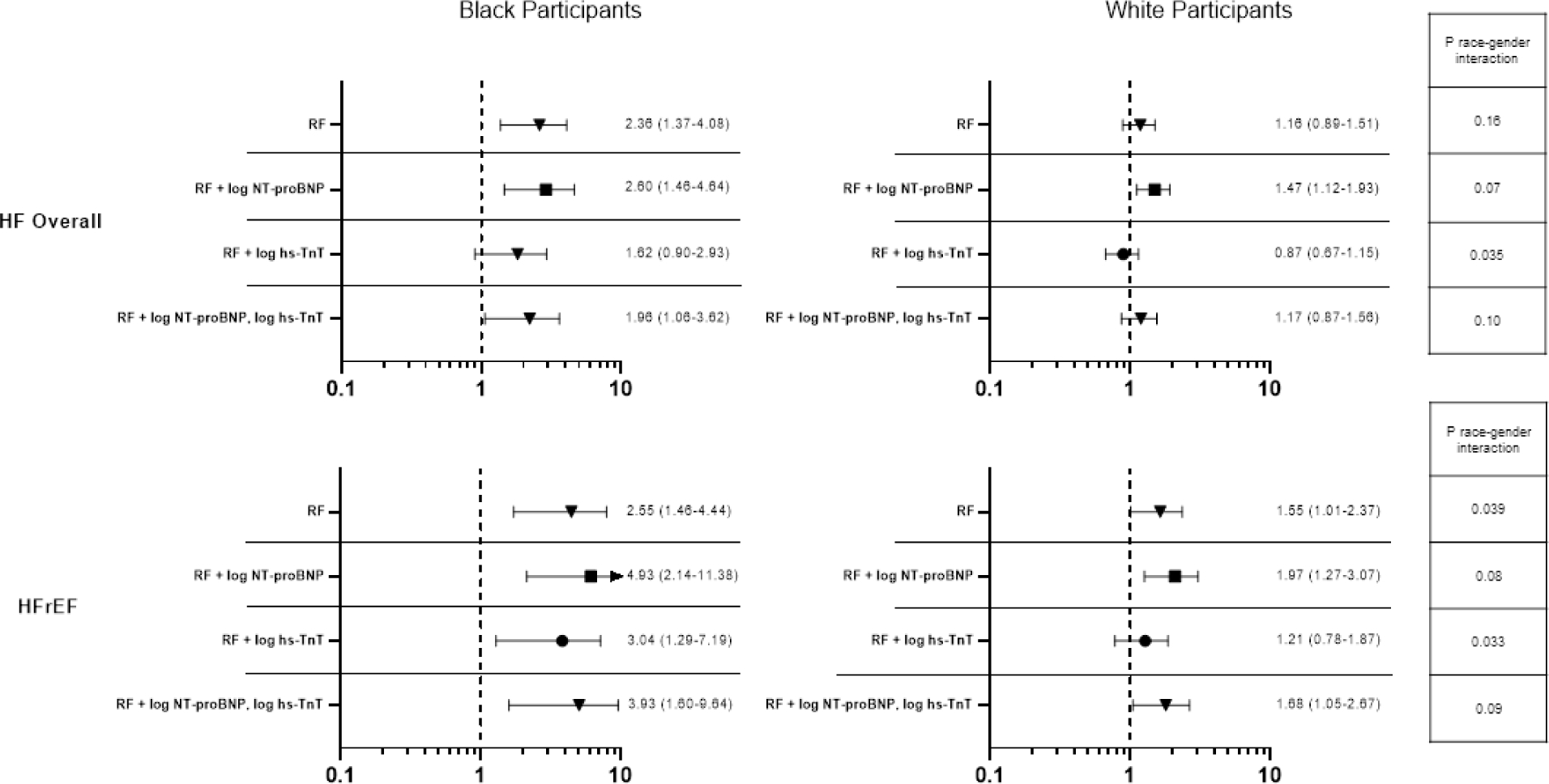
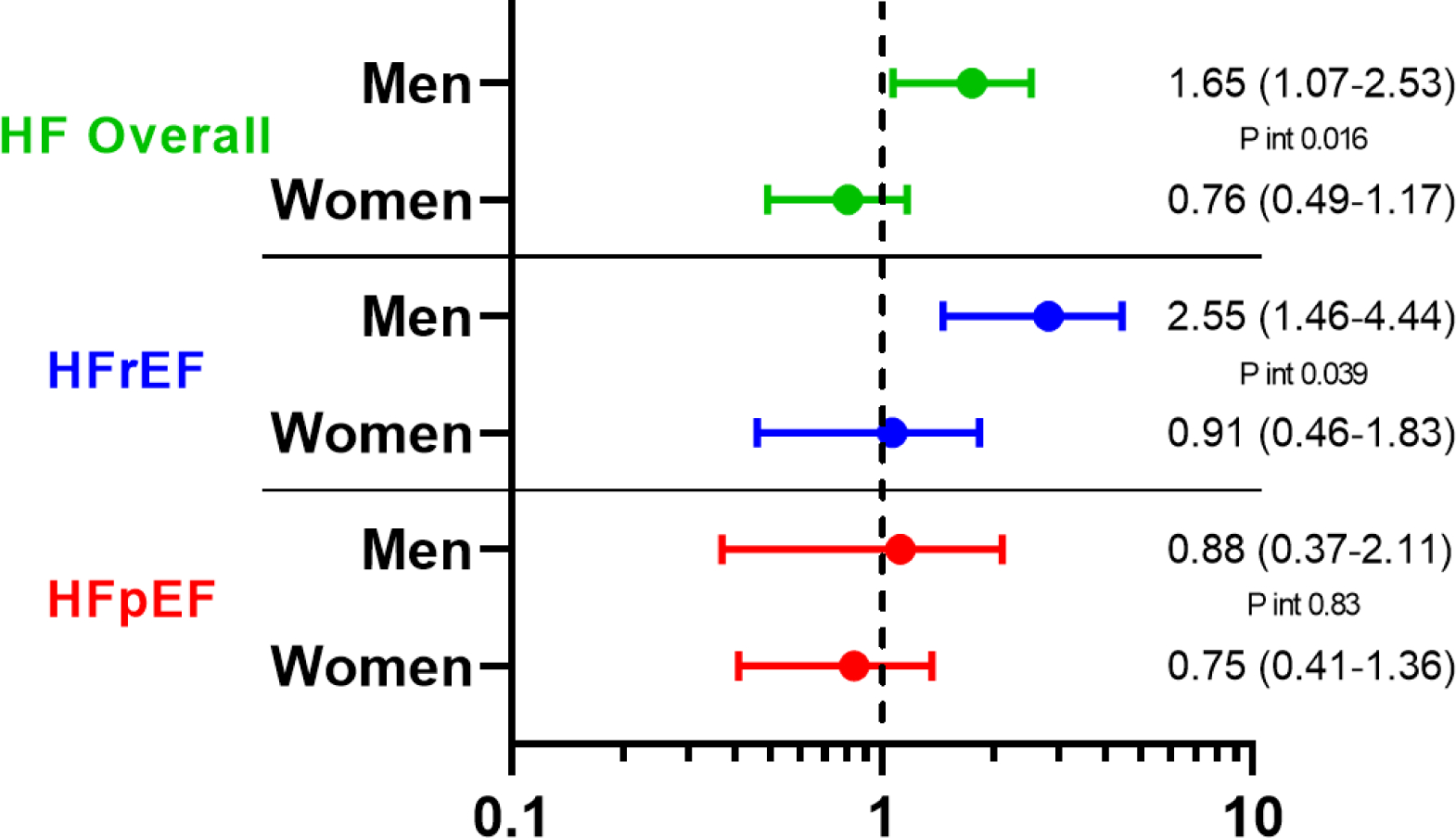
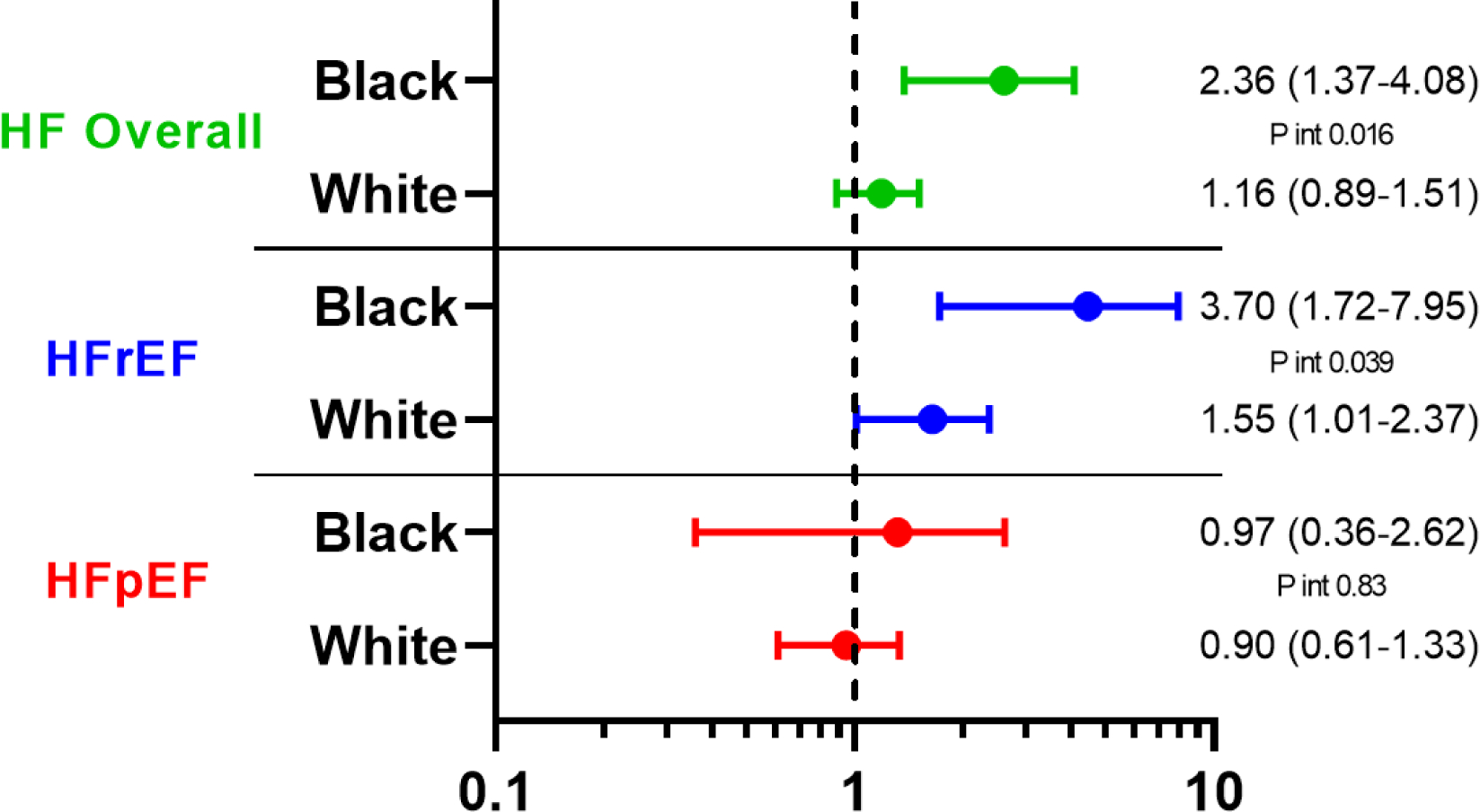
Results: Patients' mean age was 75 ± 5 years, 59% were women, and 20% were Black. Male gender and Black race were associated with lower mean left ventricular ejection fraction. Black race was also associated with greater left ventricular wall thickness and concentricity, differences that persisted after adjusting for cardiovascular comorbidities. After adjusting for cardiovascular comorbidities, men were at higher risk for HF and heart failure with reduced ejection fraction (HFrEF) in Black participants compared with White participants (HF: HR of 2.36 [95% CI: 1.37-4.08] vs 1.16 [95% CI: 0.89-1.51], interaction P = 0.016; HFrEF: HR of 3.70 [95% CI: 1.72-7.95] vs 1.55 [95% CI: 1.01-2.37] respectively, interaction P = 0.039). Black race was associated with a higher incidence of HF overall and HFrEF in men only (HF: 1.65 [95% CI: 1.07-2.53] vs 0.76 [95% CI: 0.49-1.17]; HFrEF: HR of 2.55 [95% CI: 1.46-4.44] vs 0.91 [95% CI: 0.46-1.83]). No race/gender-based differences were observed in risk of incident heart failure with preserved ejection fraction.
Conclusions: Among older persons free of HF, men and Black participants exhibit worse systolic performance and are at heightened risk for HFrEF, whereas the risk of heart failure with preserved ejection fraction is similar across gender and race groups.
Keywords: echocardiography; elderly; gender; heart failure; race.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The ARIC study has been funded in whole or in part with federal funds from the National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH), Department of Health and Human Services (HHSN268201700001I, HHSN268201700002I, HHSN268201700003I, HHSN268201700005I, and HHSN268201700004I). Dr Shah was supported by NIH/NHLBI grants R01HL135008, R01HL143224, R01HL150342, R01HL148218, and K24HL152008. Dr Chandra was supported by NIH grant 5T32HL094301-08. Dr Shah has received research support from Novartis and Philips Ultrasound through the Brigham and Women’s Hospital; and has received consulting fees from Philips Ultrasound and Edwards Lifesciences. Dr Solomon has received research grants from Alnylam, Amgen, AstraZeneca, Bellerophon, Bayer, BMS, Celladon, Cytokinetics, Eidos, Gilead, GSK, Ionis, Lone Star Heart, Mesoblast, MyoKardia, NIH/NHLBI, Novartis, Sanofi Pasteur, and Theracos; and has consulted for Akros, Alnylam, Amgen, Arena, AstraZeneca, Bayer, BMS, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi-Sankyo, Gilead, GSK, Ironwood, Merck, MyoKardia, Novartis, Roche, Takeda, Theracos, Quantum Genetics, Cardurion, AoBiome, Janssen, Cardiac Dimensions, Tenaya, Dinaqor, and Tremeau. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

Comment in
-
The Path to Better Understanding Heart Failure Epidemiology.J Am Coll Cardiol. 2022 Feb 1;79(4):369-371. doi: 10.1016/j.jacc.2021.11.025. J Am Coll Cardiol. 2022. PMID: 35086659 No abstract available.
References
-
- Croft JB, Giles WH, Pollard RA, Keenan NL, Casper ML, Anda RF. Heart failure survival among older adults in the United States: a poor prognosis for an emerging epidemic in the Medicare population. Arch Intern Med. 1999;159:505–510. - PubMed
-
- Tighe D, Brest AN. Congestive heart failure in the elderly. CardiovascClin 1992;22:127–38. - PubMed
-
- Carnethon MR, Pu J, Howard G, et al. Cardiovascular health in African Americans: a scientific statement from the American Heart Association. Circulation. 2017. Nov 21;136(21):e393–e423. - PubMed
Publication types
MeSH terms
Grants and funding
- T32 HL094301/HL/NHLBI NIH HHS/United States
- R01 HL135008/HL/NHLBI NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- R01 HL150342/HL/NHLBI NIH HHS/United States
- R01 HL148218/HL/NHLBI NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- R01 HL143224/HL/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- K24 HL152008/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
