

Clinical trial diversity: An opportunity for improved insight into the determinants of variability in drug response
- PMID: 35088432
- PMCID: PMC9306578
- DOI: 10.1111/bcp.15242
Clinical trial diversity: An opportunity for improved insight into the determinants of variability in drug response
Abstract
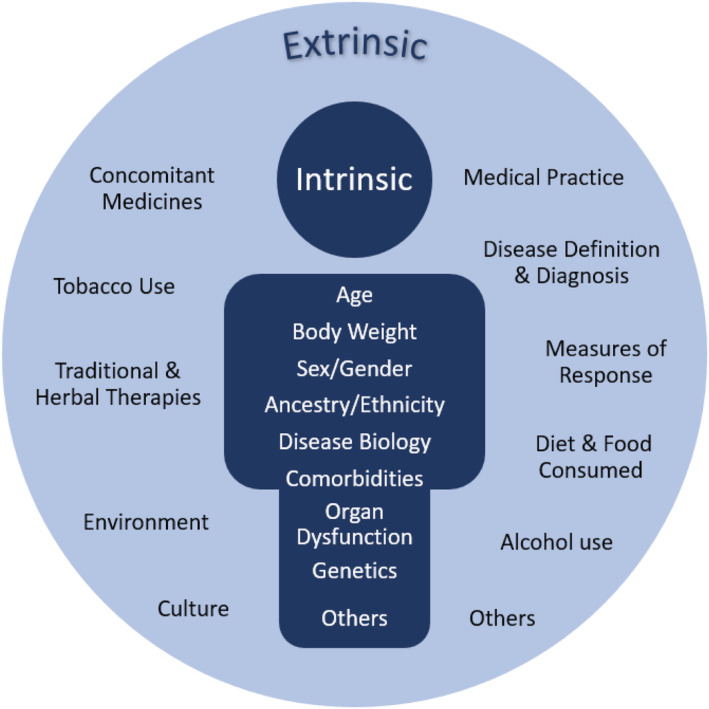
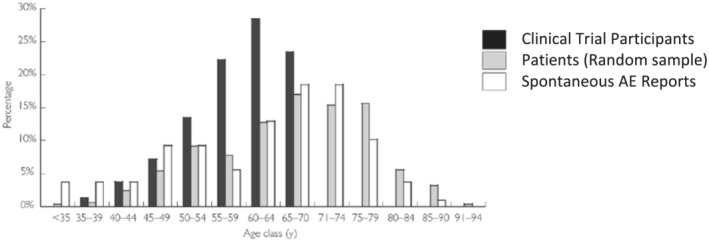
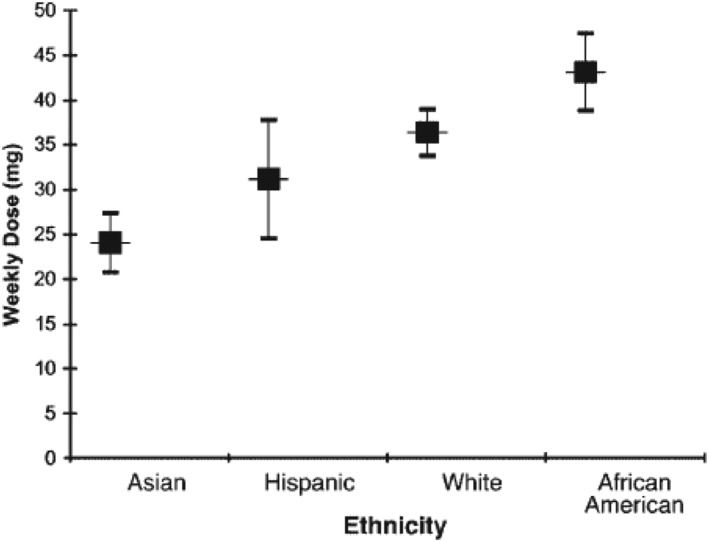
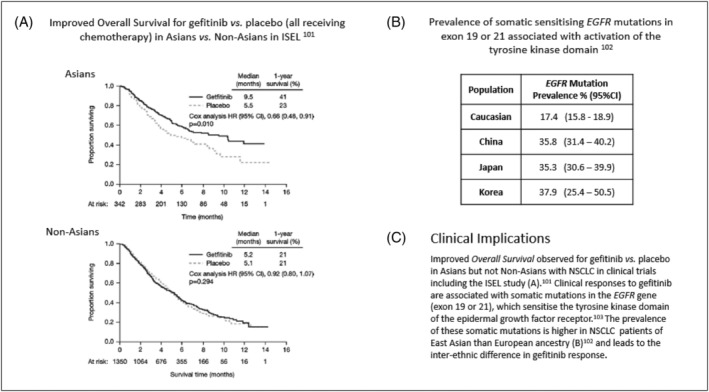
Although the number of countries participating in pivotal trials submitted to enable drug registration has nearly doubled over the past 25 years, there has not been a substantial increase in the diversity of clinical trial populations. In parallel, our understanding of factors that influence medicine response and variability has continued to evolve. The notion of intrinsic and extrinsic sources of variability has been embedded into different regulatory guidelines, including the recent guideline on the importance of enhancing the diversity of clinical trial populations. In addition to presenting the clinical and scientific reasons for ensuring that clinical trial populations represent the demographics of patient populations, this overview outlines the efforts of regulatory agencies, patient advocacy groups and clinical researchers to attain this goal through strategies to meet representation in recruitment targets and broaden eligibility criteria. Despite these efforts, challenges to participation in clinical trials remain, and certain groups continue to be underrepresented in development programmes. These challenges are amplified when the representativeness of specific groups may vary across countries and regions in a global clinical programme. Whilst enhanced trial diversity is a critical step towards ensuring that results will be representative of patient populations, a concerted effort is required to characterise further the factors influencing interindividual and regional differences in response for global populations. Quantitative clinical pharmacology principles should be applied to allow extrapolation of data across groups or regions as well as provide insight into the effect of patient-specific characteristics on a medicine's dose rationale and efficacy and safety profiles.
Keywords: age; diversity; ethnicity; recruitment; sex.
© 2022 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
The authors have no conflicts of interest to disclose in addition to their affiliation with GSK.
Figures


References
-
- International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use . ICH Harmonised Tripartite Guideline. ICH E5 (R1): Ethnic Factors in the Acceptability of Foreign Clinical Data. 1998. Accessed August 5, 2020. https://database.ich.org/sites/default/files/E5_R1__Guideline.pdf
-
- International Council on Harmonisation of Technical Requirements for Pharmaceuticals for Human Use . ICH Harmonised Guidelines. General Principles for Planning and Design of Multi‐Regional Clinical Trials. ICH E17. 2017. Accessed October 6, 2020. https://database.ich.org/sites/default/files/E17EWG_Step4_2017_1116.pdf
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
