

APOL1 Risk Variants, Acute Kidney Injury, and Death in Participants With African Ancestry Hospitalized With COVID-19 From the Million Veteran Program
- PMID: 35089317
- PMCID: PMC8980930
- DOI: 10.1001/jamainternmed.2021.8538
APOL1 Risk Variants, Acute Kidney Injury, and Death in Participants With African Ancestry Hospitalized With COVID-19 From the Million Veteran Program
Abstract
Importance: Coronavirus disease 2019 (COVID-19) confers significant risk of acute kidney injury (AKI). Patients with COVID-19 with AKI have high mortality rates.
Objective: Individuals with African ancestry with 2 copies of apolipoprotein L1 (APOL1) variants G1 or G2 (high-risk group) have significantly increased rates of kidney disease. We tested the hypothesis that the APOL1 high-risk group is associated with a higher-risk of COVID-19-associated AKI and death.
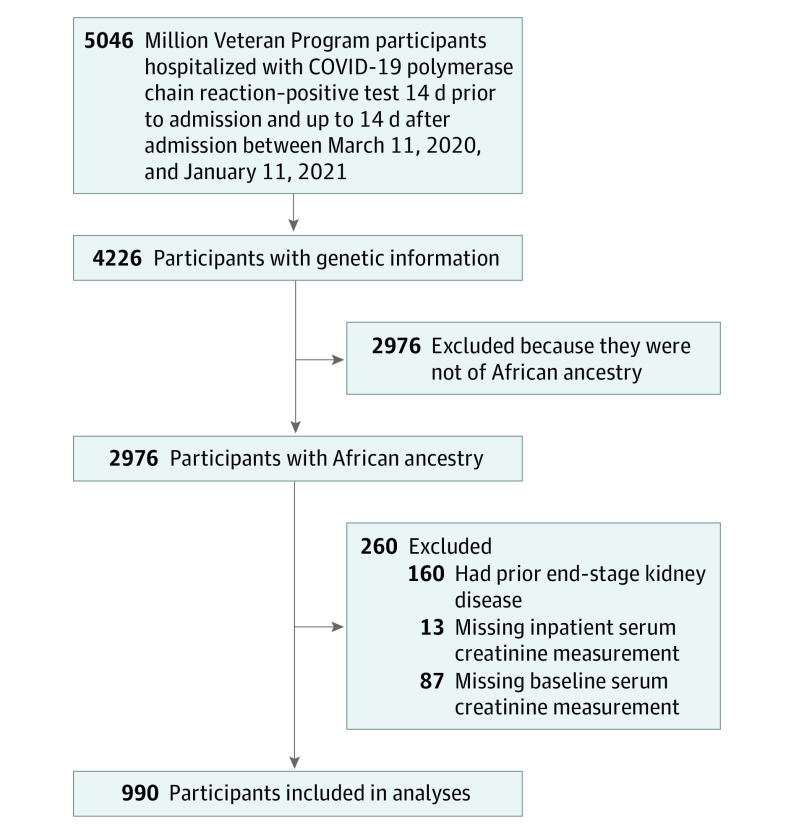
Design, setting, and participants: This retrospective cohort study included 990 participants with African ancestry enrolled in the Million Veteran Program who were hospitalized with COVID-19 between March 2020 and January 2021 with available genetic information.
Exposures: The primary exposure was having 2 APOL1 risk variants (RV) (APOL1 high-risk group), compared with having 1 or 0 risk variants (APOL1 low-risk group).
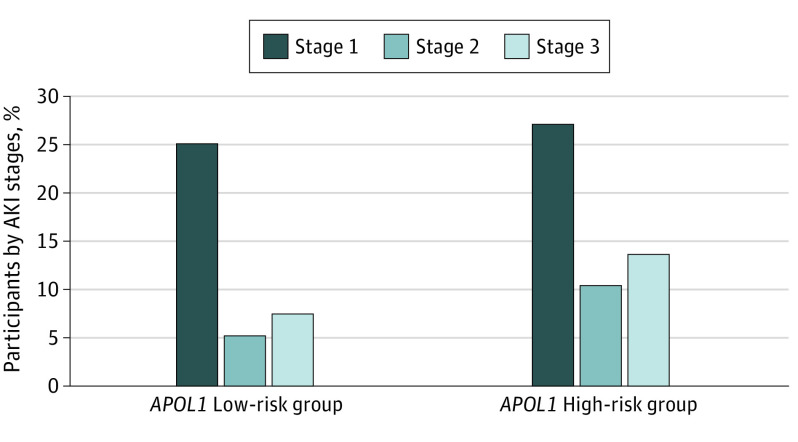
Main outcomes and measures: The primary outcome was AKI. The secondary outcomes were stages of AKI severity and death. Multivariable logistic regression analyses adjusted for preexisting comorbidities, medications, and inpatient AKI risk factors; 10 principal components of ancestry were performed to study these associations. We performed a subgroup analysis in individuals with normal kidney function prior to hospitalization (estimated glomerular filtration rate ≥60 mL/min/1.73 m2).
Results: Of the 990 participants with African ancestry, 905 (91.4%) were male with a median (IQR) age of 68 (60-73) years. Overall, 392 (39.6%) patients developed AKI, 141 (14%) developed stages 2 or 3 AKI, 28 (3%) required dialysis, and 122 (12.3%) died. One hundred twenty-five (12.6%) of the participants were in the APOL1 high-risk group. Patients categorized as APOL1 high-risk group had significantly higher odds of AKI (adjusted odds ratio [OR], 1.95; 95% CI, 1.27-3.02; P = .002), higher AKI severity stages (OR, 2.03; 95% CI, 1.37-2.99; P < .001), and death (OR, 2.15; 95% CI, 1.22-3.72; P = .007). The association with AKI persisted in the subgroup with normal kidney function (OR, 1.93; 95% CI, 1.15-3.26; P = .01). Data analysis was conducted between February 2021 and April 2021.
Conclusions and relevance: In this cohort study of veterans with African ancestry hospitalized with COVID-19 infection, APOL1 kidney risk variants were associated with higher odds of AKI, AKI severity, and death, even among individuals with prior normal kidney function.
Conflict of interest statement
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
