

Symptoms Compatible With Long Coronavirus Disease (COVID) in Healthcare Workers With and Without Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection-Results of a Prospective Multicenter Cohort
- PMID: 35090015
- PMCID: PMC9383387
- DOI: 10.1093/cid/ciac054
Symptoms Compatible With Long Coronavirus Disease (COVID) in Healthcare Workers With and Without Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection-Results of a Prospective Multicenter Cohort
Abstract
Background: The burden of long-term symptoms (ie, long COVID) in patients after mild COVID-19 is debated. Within a cohort of healthcare workers (HCWs), frequency and risk factors for symptoms compatible with long COVID are assessed.
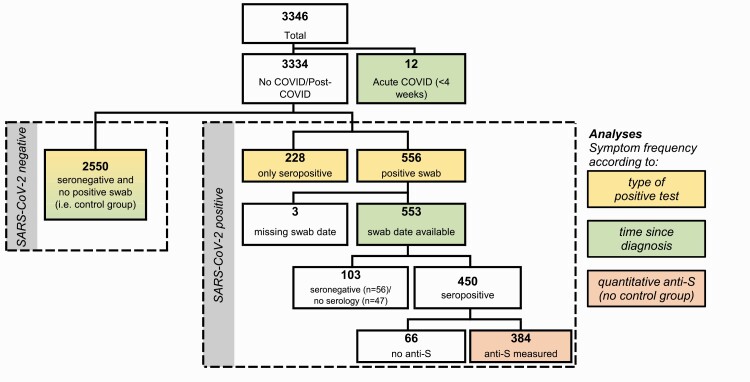
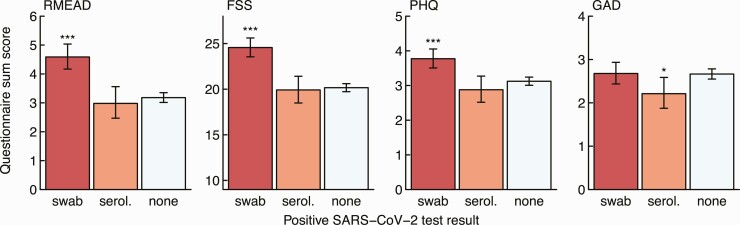
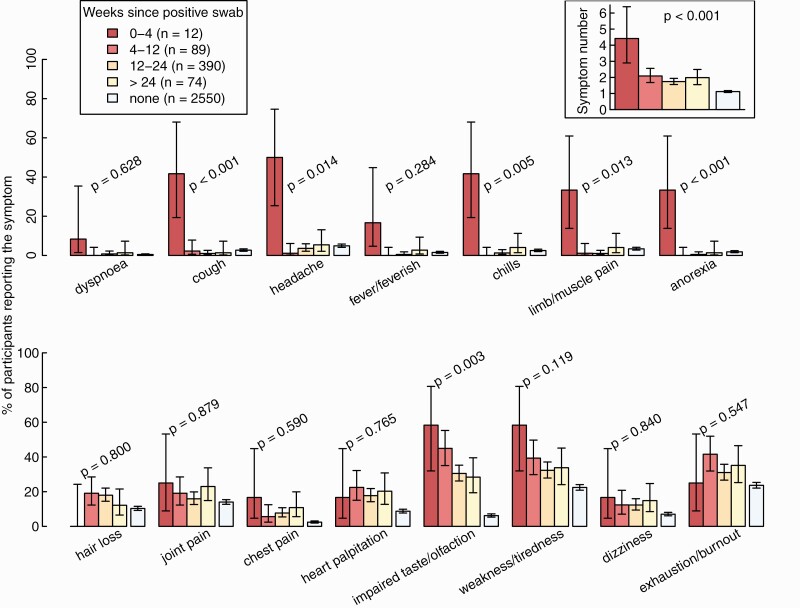
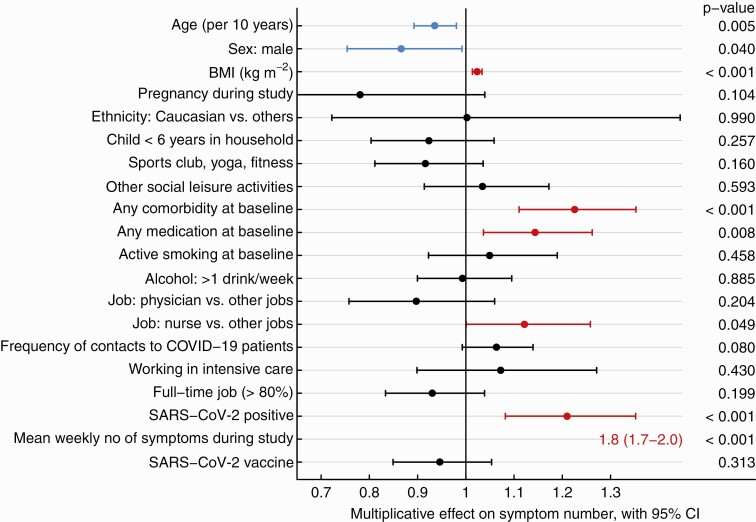
Methods: Participants answered baseline (August/September 2020) and weekly questionnaires on SARS-CoV-2 nasopharyngeal swab (NPS) results and acute disease symptoms. In January 2021, SARS-CoV-2 serology was performed; in March, symptoms compatible with long COVID (including psychometric scores) were asked and compared between HCWs with positive NPS, seropositive HCWs without positive NPS (presumable asymptomatic/pauci-symptomatic infections), and negative controls. The effect of time since diagnosis and quantitative anti-spike protein antibodies (anti-S) was evaluated. Poisson regression was used to identify risk factors for symptom occurrence.
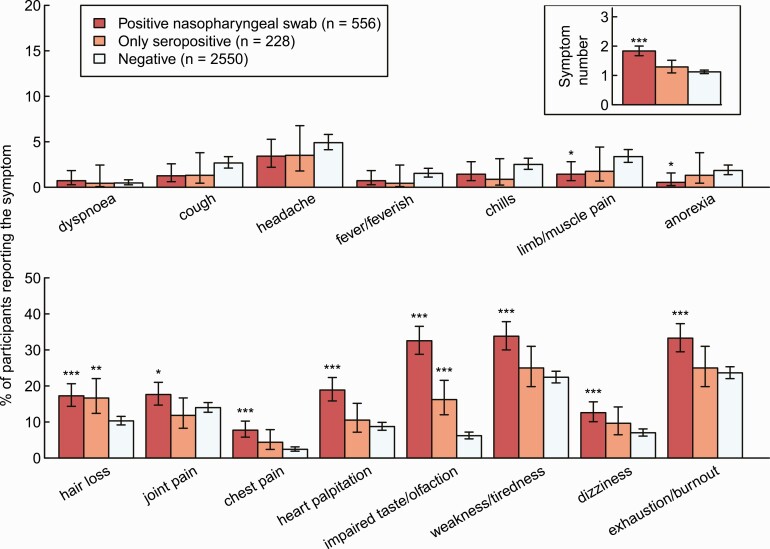
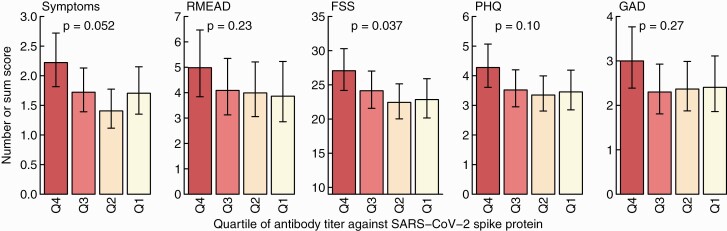
Results: Of 3334 HCWs (median, 41 years; 80% female), 556 (17%) had a positive NPS and 228 (7%) were only seropositive. HCWs with positive NPS more frequently reported ≥1 symptom compared with controls (73% vs 52%, P < .001); seropositive HCWs without positive NPS did not score higher than controls (58% vs 52%, P = .13), although impaired taste/olfaction (16% vs 6%, P < .001) and hair loss (17% vs 10%, P = .004) were more common. Exhaustion/burnout was reported by 24% of negative controls. Many symptoms remained elevated in those diagnosed >6 months ago; anti-S titers correlated with high symptom scores. Acute viral symptoms in weekly questionnaires best predicted long-COVID symptoms. Physical activity at baseline was negatively associated with neurocognitive impairment and fatigue scores.
Conclusions: Seropositive HCWs without positive NPS are only mildly affected by long COVID. Exhaustion/burnout is common, even in noninfected HCWs. Physical activity might be protective against neurocognitive impairment/fatigue symptoms after COVID-19.
Keywords: asymptomatic; healthcare workers; long COVID; risk factors; serology.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Ayoubkhani D. Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK: 1 April 2021. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/.... Accessed 22 July 2021.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
