

Effects of Balance Exercise Assist Robot training for patients with hemiparetic stroke: a randomized controlled trial
- PMID: 35090517
- PMCID: PMC8796441
- DOI: 10.1186/s12984-022-00989-6
Effects of Balance Exercise Assist Robot training for patients with hemiparetic stroke: a randomized controlled trial
Abstract
Background: Robot-assisted rehabilitation for patients with stroke is promising. However, it is unclear whether additional balance training using a balance-focused robot combined with conventional rehabilitation programs supplements the balance function in patients with stroke. The purpose of this study was to compare the effects of Balance Exercise Assist Robot (BEAR) training combined with conventional inpatient rehabilitation training to those of conventional inpatient rehabilitation only in patients with hemiparetic stroke. We also aimed to determine whether BEAR training was superior to intensive balance training.
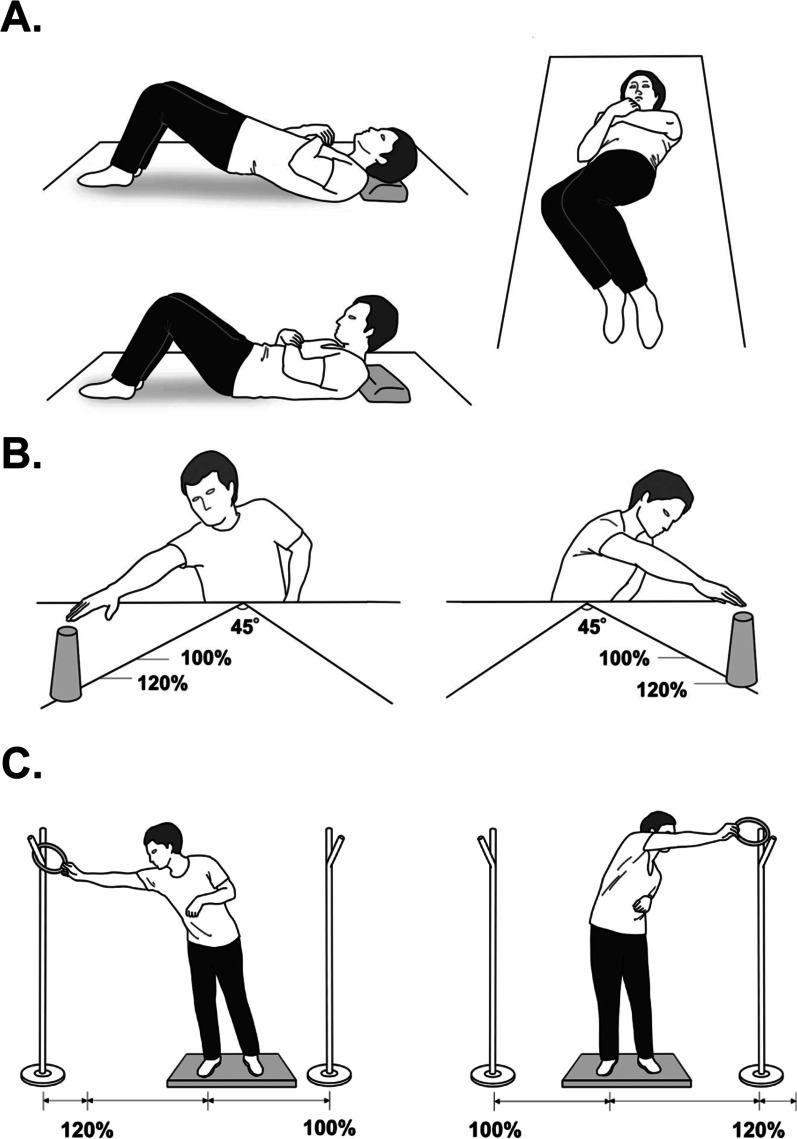
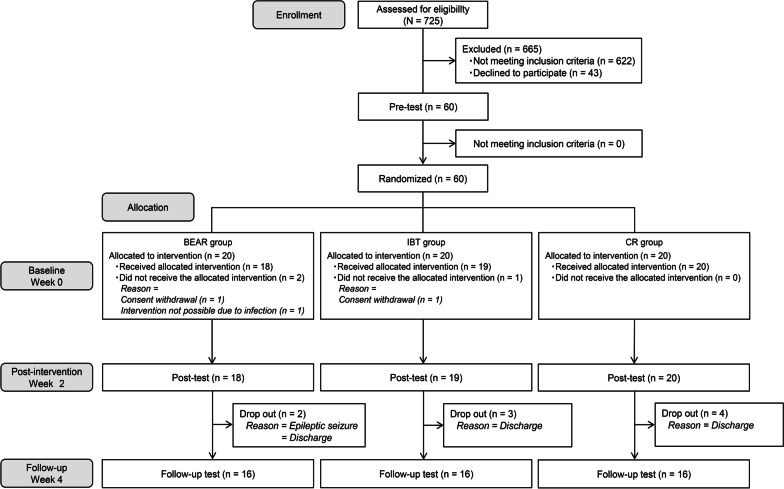
Methods: This assessor-blinded randomized controlled trial included 60 patients with first-ever hemiparetic stroke, admitted to rehabilitation wards between December 2016 and February 2019. Patients were randomly assigned to one of three groups, robotic balance training and conventional inpatient rehabilitation (BEAR group), intensive balance training and conventional inpatient rehabilitation (IBT group), or conventional inpatient rehabilitation-only (CR group). The intervention duration was 2 weeks, with assessments conducted pre- and post-intervention, and at 2 weeks follow-up. The primary outcome measure was a change in the Mini-Balance Evaluation Systems Test (Mini-BESTest) score from baseline.
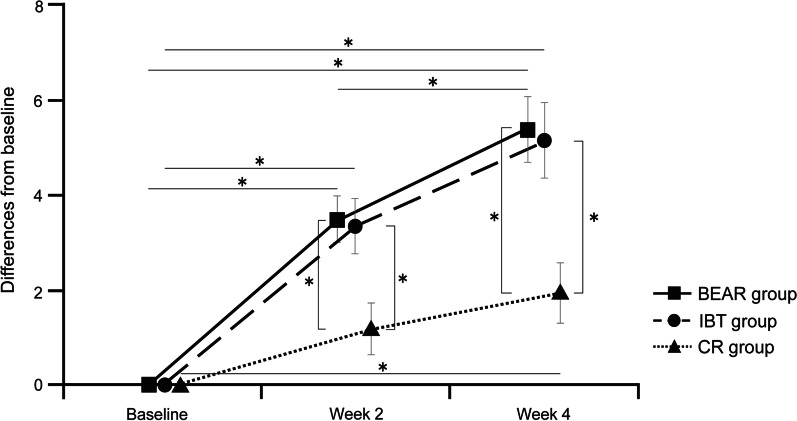
Results: In total, 57 patients completed the intervention, and 48 patients were evaluated at the follow-up. Significant improvements in Mini-BESTest score were observed in the BEAR and IBT groups compared with in the CR group post-intervention and after the 2-week follow-up period (P < 0.05).
Conclusions: The addition of balance exercises using the BEAR alongside conventional inpatient rehabilitation improved balance in patients with subacute stroke.
Trial registration: https://www.umin.ac.jp/ctr ; Unique Identifier: UMIN000025129. Registered on 2 December 2016.
Keywords: Cerebrovascular disorder; Exercise; Physical therapy; Postural balance; Rehabilitation; Robotics.
© 2022. The Author(s).
Conflict of interest statement
YO was appointed at his current institution, the Fujita Health University, in April 2017. The institution has received research funding from the TOYOTA Motor Corporation, which developed the BEAR. However, no support was obtained for the present study, which was started in 2016 and conducted in another institution, Tokyo Bay Rehabilitation Hospital. All other authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
