

Safety and immunogenicity of an AS03-adjuvanted SARS-CoV-2 recombinant protein vaccine (CoV2 preS dTM) in healthy adults: interim findings from a phase 2, randomised, dose-finding, multicentre study
- PMID: 35090638
- PMCID: PMC8789245
- DOI: 10.1016/S1473-3099(21)00764-7
Safety and immunogenicity of an AS03-adjuvanted SARS-CoV-2 recombinant protein vaccine (CoV2 preS dTM) in healthy adults: interim findings from a phase 2, randomised, dose-finding, multicentre study
Abstract
Background: We evaluated our SARS-CoV-2 prefusion spike recombinant protein vaccine (CoV2 preS dTM) with different adjuvants, unadjuvanted, and in a one-injection and two-injection dosing schedule in a previous phase 1-2 study. Based on interim results from that study, we selected a two-injection schedule and the AS03 adjuvant for further clinical development. However, lower than expected antibody responses, particularly in older adults, and higher than expected reactogenicity after the second vaccination were observed. In the current study, we evaluated the safety and immunogenicity of an optimised formulation of CoV2 preS dTM adjuvanted with AS03 to inform progression to phase 3 clinical trial.
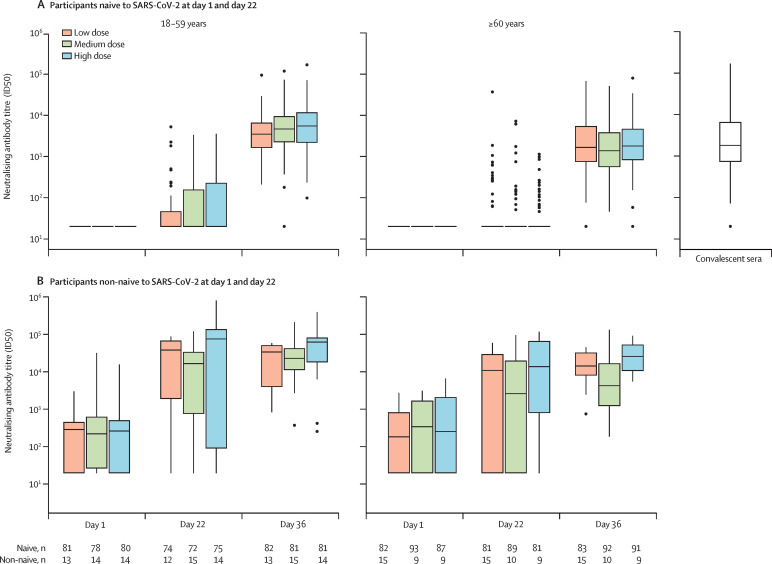
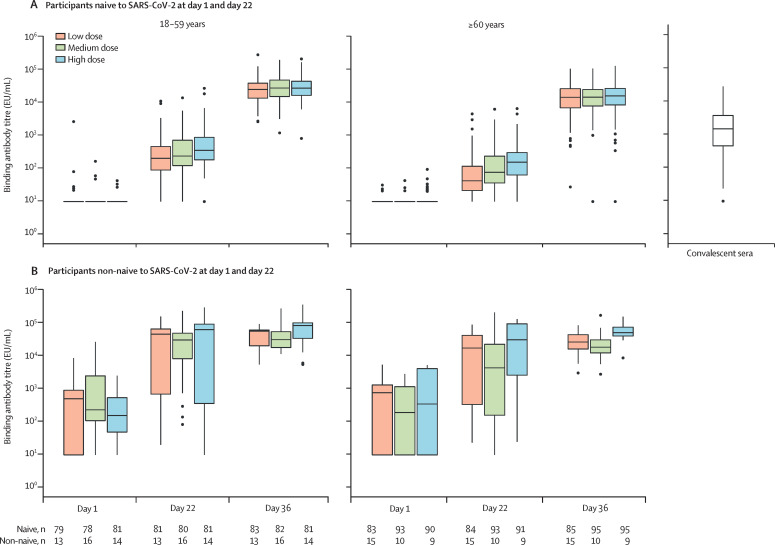
Methods: This phase 2, randomised, parallel-group, dose-ranging study was done in adults (≥18 years old), including those with pre-existing medical conditions, those who were immunocompromised (except those with recent organ transplant or chemotherapy) and those with a potentially increased risk for severe COVID-19, at 20 clinical research centres in the USA and Honduras. Women who were pregnant or lactating or, for those of childbearing potential, not using an effective method of contraception or abstinence, and those who had received a COVID-19 vaccine, were excluded. Participants were randomly assigned (1:1:1) using an interactive response technology system, with stratification by age (18-59 years and ≥60 years), rapid serodiagnostic test result (positive or negative), and high-risk medical conditions (yes or no), to receive two injections (day 1 and day 22) of 5 7mu;g (low dose), 10 7mu;g (medium dose), or 15 7mu;g (high dose) CoV2 preS dTM antigen with fixed AS03 content. All participants and outcome assessors were masked to group assignment; unmasked study staff involved in vaccine preparation were not involved in safety outcome assessments. All laboratory staff performing the assays were masked to treatment. The primary safety objective was to describe the safety profile in all participants, for each candidate vaccine formulation. Safety endpoints were evaluated for all randomised participants who received at least one dose of the study vaccine (safety analysis set), and are presented here for the interim study period (up to day 43). The primary immunogenicity objective was to describe the neutralising antibody titres to the D614G variant 14 days after the second vaccination (day 36) in participants who were SARS-CoV-2 naive who received both injections, provided samples at day 1 and day 36, did not have protocol deviations, and did not receive an authorised COVID-19 vaccine before day 36. Neutralising antibodies were measured using a pseudovirus neutralisation assay and are presented here up to 14 days after the second dose. As a secondary immunogenicity objective, we assessed neutralising antibodies in non-naive participants. This trial is registered with ClinicalTrials.gov (NCT04762680) and is closed to new participants for the cohort reported here.
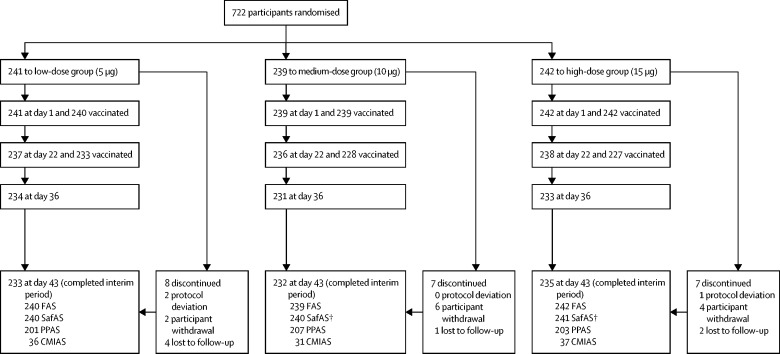
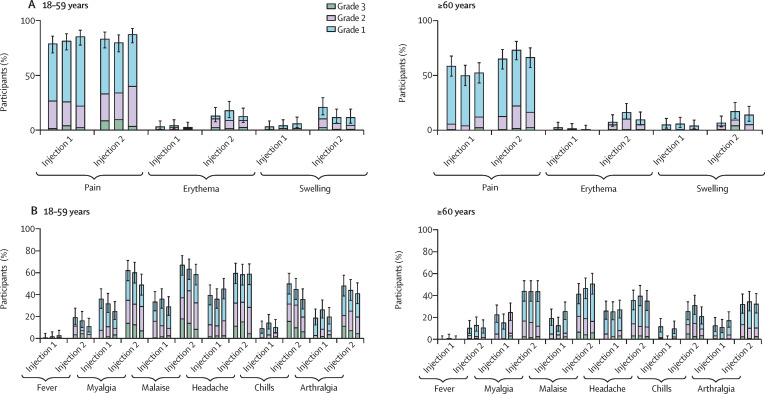
Findings: Of 722 participants enrolled and randomly assigned between Feb 24, 2021, and March 8, 2021, 721 received at least one injection (low dose=240, medium dose=239, and high dose=242). The proportion of participants reporting at least one solicited adverse reaction (injection site or systemic) in the first 7 days after any vaccination was similar between treatment groups (217 [91%] of 238 in the low-dose group, 213 [90%] of 237 in the medium-dose group, and 218 [91%] of 239 in the high-dose group); these adverse reactions were transient, were mostly mild to moderate in intensity, and occurred at a higher frequency and intensity after the second vaccination. Four participants reported immediate unsolicited adverse events; two (one each in the low-dose group and medium-dose group) were considered by the investigators to be vaccine related and two (one each in the low-dose and high-dose groups) were considered unrelated. Five participants reported seven vaccine-related medically attended adverse events (two in the low-dose group, one in the medium-dose group, and four in the high-dose group). No vaccine-related serious adverse events and no adverse events of special interest were reported. Among participants naive to SARS-CoV-2 at day 36, 158 (98%) of 162 in the low-dose group, 166 (99%) of 168 in the medium-dose group, and 163 (98%) of 166 in the high-dose group had at least a two-fold increase in neutralising antibody titres to the D614G variant from baseline. Neutralising antibody geometric mean titres (GMTs) at day 36 for participants who were naive were 2189 (95% CI 1744-2746) for the low-dose group, 2269 (1792-2873) for the medium-dose group, and 2895 (2294-3654) for the high-dose group. GMT ratios (day 36: day 1) were 107 (95% CI 85-135) in the low-dose group, 110 (87-140) in the medium-dose group, and 141 (111-179) in the high-dose group. Neutralising antibody titres in non-naive adults 21 days after one injection tended to be higher than titres after two injections in adults who were naive, with GMTs 21 days after one injection for participants who were non-naive being 3143 (95% CI 836-11 815) in the low-dose group, 2338 (593-9226) in the medium-dose group, and 7069 (1361-36 725) in the high-dose group.
Interpretation: Two injections of CoV2 preS dTM-AS03 showed acceptable safety and reactogenicity, and robust immunogenicity in adults who were SARS-CoV-2 naive and non-naive. These results supported progression to phase 3 evaluation of the 10 7mu;g antigen dose for primary vaccination and a 5 7mu;g antigen dose for booster vaccination.
Funding: Sanofi Pasteur and Biomedical Advanced Research and Development Authority.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SSr, MIB, A-LC, AC, RMC, BF, HJ, YM, ER, NR, DvB, GdB, RC, M-HG, DL, RM, SM, CM, CAD, and SSa are Sanofi Pasteur employees. SSr, MIB, HJ, CM, and SSa own stock or stock options; A-LC, NR, and M-HG hold shares or restricted shares; and RMC reports owning shareholder and vesting options in Sanofi Pasteur. SSr, RMC, GdB, CAD, and SSa are inventors on a pending patent application filed by Sanofi Pasteur and GlaxoSmithKline (GSK) for the development of the CoV-2 dTM vaccine. LS, MK, MAC, and FT-D-S are employed by, and hold restricted shares in, the GSK group of companies. AJ was contracted by Sanofi Pasteur. DD received funding from Sanofi Pasteur for his institution, George Washington University, to serve as a clinical site for the vaccine trial. NG reports receiving funding and study materials from Sanofi and funding from the National Institute of Allergy and Infectious Diseases (NIAID) through the COVID-19 Prevention Network (CoVPN), which provides research grants to her institution, the Fred Hutchinson Cancer Research Center. MCK received NIAID funding support for the current study, paid to the clinical trials site for the CoVPN and HIV vaccine trials network; Sanofi Pasteur contracted the site to do this clinical trial. DMRM received a research grant from Sanofi Pasteur for this study. OO received a Gilead Sciences grant paid to Yale, and consulting fees from Gilead Sciences. OO also reports that Gilead, Integrity CE, and Medscape paid for lectures, presentations, manuscript writing, or educational events and that Gilead and ViiV Healthcare paid for their participation on a data safety monitoring or advisory board. VNR received funding from Sanofi for the CoVPN and Vaccine Treatment and Evaluation Units for COVID-19 vaccine clinical trials, and payments from Pfizer to her institution for the conduct of COVID-19 vaccine clinical trials. RS received clinical trial investigator site contracts with AES Synexus. NGR received a grant from Sanofi Pasteur to do this study and received grants from Sanofi, Merck, Pfizer, Quidel, and Lilly in the past 36 months. NGR received a payment from the Infectious Disease Association of California and participated on advisory or safety monitoring boards for Micron, ICON, and The Emmes Company; NGR also reports having a leadership or fiduciary role (paid or unpaid) for the Infectious Diseases Society of America, the Vaccine Treatment and Evaluation Unit and Antibacterial Resistance Leadership Group. LDS received a research grant from Sanofi Pasteur and SRW and JW were contracted by Sanofi Pasteur. AB, BJE, NLM, SSM, MKJ, SR, JS, TT, and JT declare no competing interests.
Figures
References
-
- World Bank . World Bank; Washington, DC: 2021. Global economic prospects, June 2021.
-
- WHO The impact of COVID-19 on global health goals. https://www.who.int/news-room/spotlight/the-impact-of-covid-19-on-global...
-
- Regulatory Affairs Professionals Society COVID-19 vaccine tracker. https://www.raps.org/news-and-articles/news-articles/2020/3/covid-19-vac...
-
- Arunachalam PS, Walls AC, Golden N, et al. Adjuvanting a subunit COVID-19 vaccine to induce protective immunity. Nature. 2021;594:253–258. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
