

Continuous real-time prediction of surgical case duration using a modular artificial neural network
- PMID: 35090725
- PMCID: PMC9074795
- DOI: 10.1016/j.bja.2021.12.039
Continuous real-time prediction of surgical case duration using a modular artificial neural network
Abstract
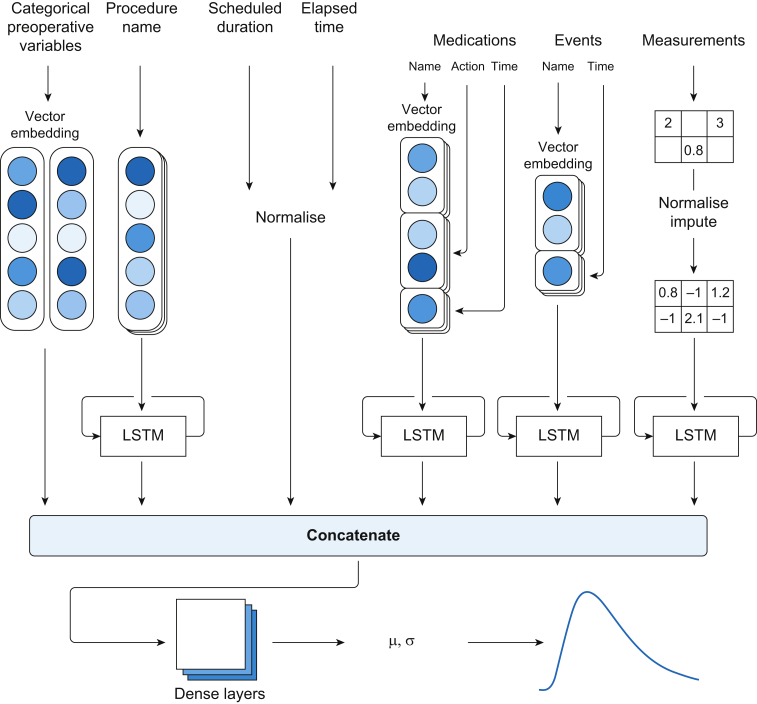
Background: Real-time prediction of surgical duration can inform perioperative decisions and reduce surgical costs. We developed a machine learning approach that continuously incorporates preoperative and intraoperative information for forecasting surgical duration.
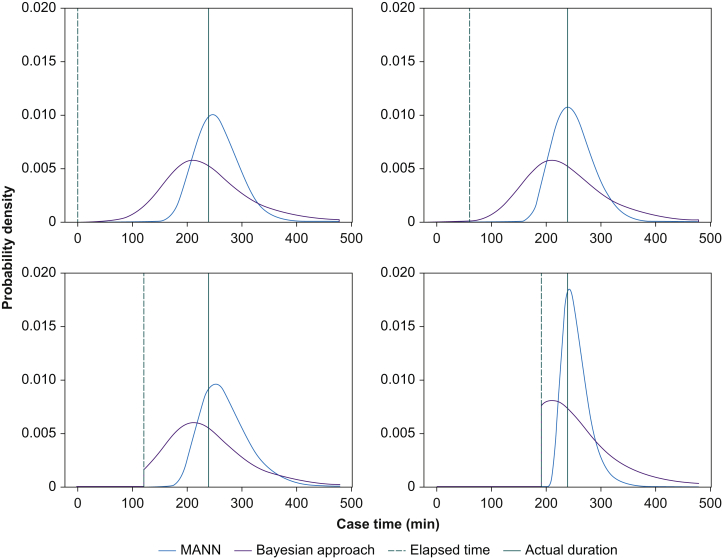
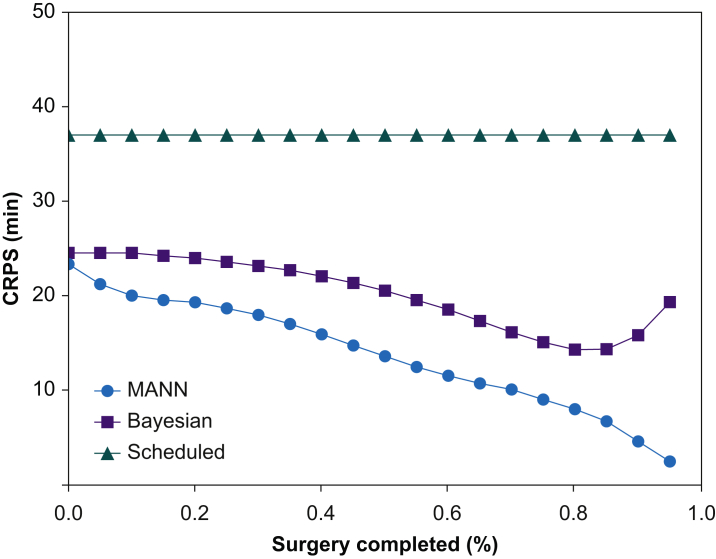
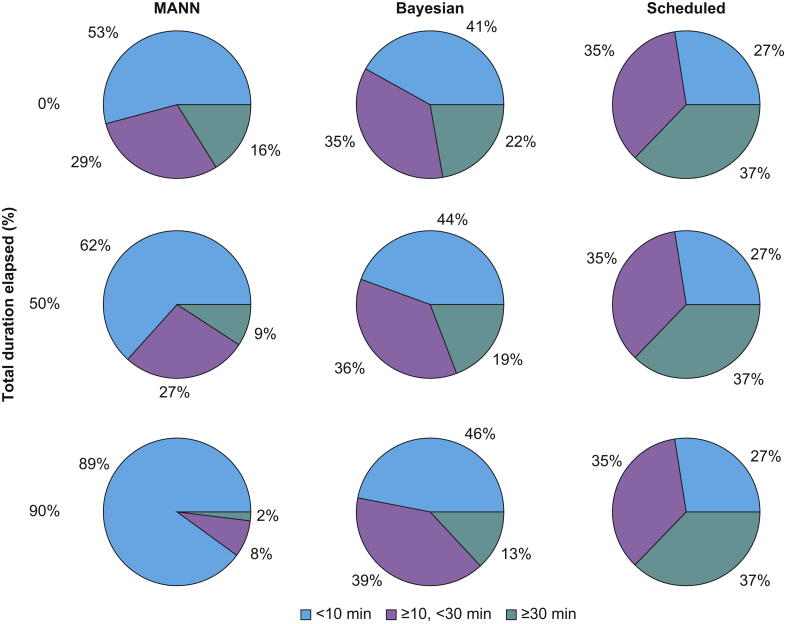
Methods: Preoperative (e.g. procedure name) and intraoperative (e.g. medications and vital signs) variables were retrieved from anaesthetic records of surgeries performed between March 1, 2019 and October 31, 2019. A modular artificial neural network was developed and compared with a Bayesian approach and the scheduled surgical duration. Continuous ranked probability score (CRPS) was used as a measure of time error to assess model accuracy. For evaluating clinical performance, accuracy for each approach was assessed in identifying cases that ran beyond 15:00 (commonly scheduled end of shift), thus identifying opportunities to avoid overtime labour costs.
Results: The analysis included 70 826 cases performed at eight hospitals. The modular artificial neural network had the lowest time error (CRPS: mean=13.8; standard deviation=35.4 min), which was significantly better (mean difference=6.4 min [95% confidence interval: 6.3-6.5]; P<0.001) than the Bayesian approach. The modular artificial neural network also had the highest accuracy in identifying operating theatres that would overrun 15:00 (accuracy at 1 h prior=89%) compared with the Bayesian approach (80%) and a naïve approach using the scheduled duration (78%).
Conclusions: A real-time neural network model using preoperative and intraoperative data had significantly better performance than a Bayesian approach or scheduled duration, offering opportunities to avoid overtime labour costs and reduce the cost of surgery by providing superior real-time information for perioperative decision support.
Keywords: artificial neural network; economics; healthcare costs; machine learning; operating theatre efficiency; procedure duration; statistical model; surgery.
Copyright © 2022 British Journal of Anaesthesia. Published by Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Case duration prediction and estimating time remaining in ongoing cases.Br J Anaesth. 2022 May;128(5):751-755. doi: 10.1016/j.bja.2022.02.002. Epub 2022 Apr 2. Br J Anaesth. 2022. PMID: 35382924
References
-
- Stey A.M., Brook R.H., Needleman J., et al. Hospital costs by cost center of inpatient hospitalization for Medicare patients undergoing major abdominal surgery. J Am Coll Surg. 2015;220:207–217.e11. - PubMed
-
- Rothstein D.H., Raval M.V. Operating room efficiency. Semin Pediatr Surg. 2018;27:79–85. - PubMed
-
- Denton B., Viapiano J., Vogl A. Optimization of surgery sequencing and scheduling decisions under uncertainty. Health Care Manag Sci. 2007;10:13–24. - PubMed
-
- Pandit J.J. Rational planning of operating lists: a prospective comparison of ‘booking to the mean’ vs. ‘probabilistic case scheduling’ in urology. Anaesthesia. 2020;75:642–647. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
