

Phase I Trial of Cetuximab, Radiotherapy, and Ipilimumab in Locally Advanced Head and Neck Cancer
- PMID: 35091445
- PMCID: PMC9164766
- DOI: 10.1158/1078-0432.CCR-21-0426
Phase I Trial of Cetuximab, Radiotherapy, and Ipilimumab in Locally Advanced Head and Neck Cancer
Abstract
Purpose: Concurrent radiotherapy with cetuximab, an anti-EGFR mAb, is a standard treatment for locally advanced head and neck squamous carcinoma (HNSCC). Cytotoxic T lymphocyte antigen-4-positive (CTLA-4+) regulatory T cells (Treg) dampen cellular immunity and correlate negatively with clinical outcomes. This phase I study added ipilimumab, an anti-CTLA-4 mAb, to cetuximab-radiotherapy.
Patients and methods: A (3 + 3) design was used to establish the recommended phase II dose (RP2D) of ipilimumab, added at week 5 for four, every-3-week doses to fixed, standard cetuximab-radiotherapy. Eligible subjects had stage III to IVb, high-risk [human papillomavirus-negative (HPV-)] or intermediate-risk HPV-positive (HPV+)] HNSCC. Dose-limiting toxicity (DLT) was defined as any grade 4 adverse event (AE) except in-field radiation dermatitis or immune-related (ir) AE requiring ≥2 weeks of systemic steroids. Baseline tumor and serial blood specimens were collected for immune correlatives.
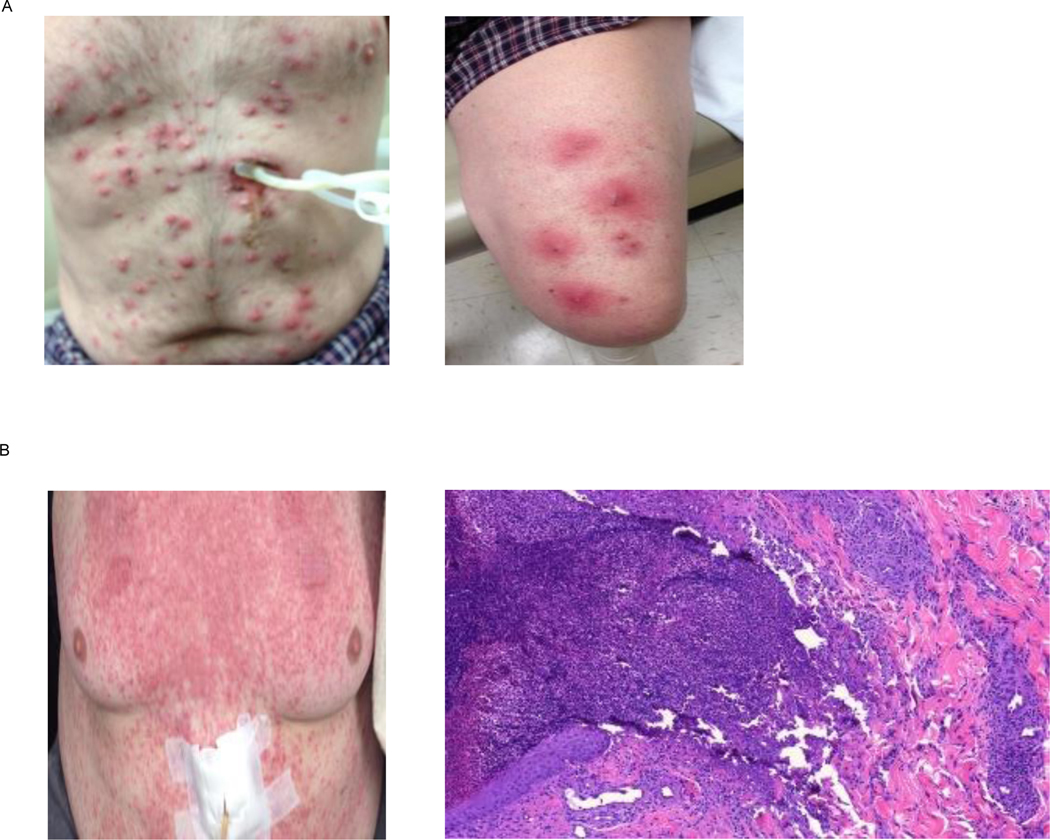
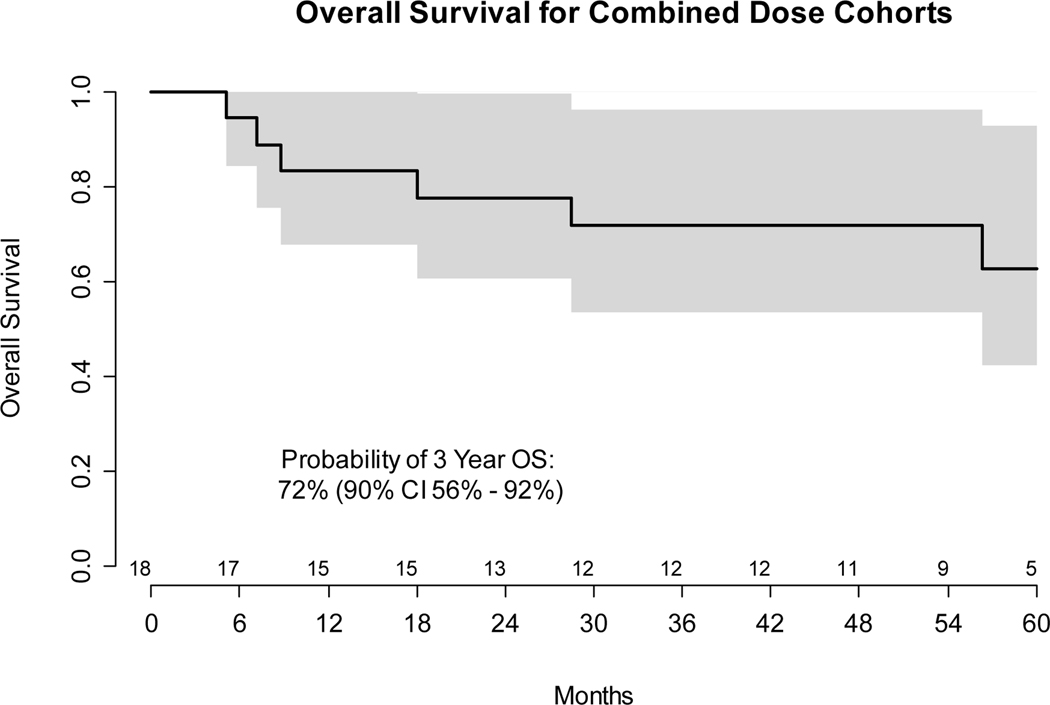
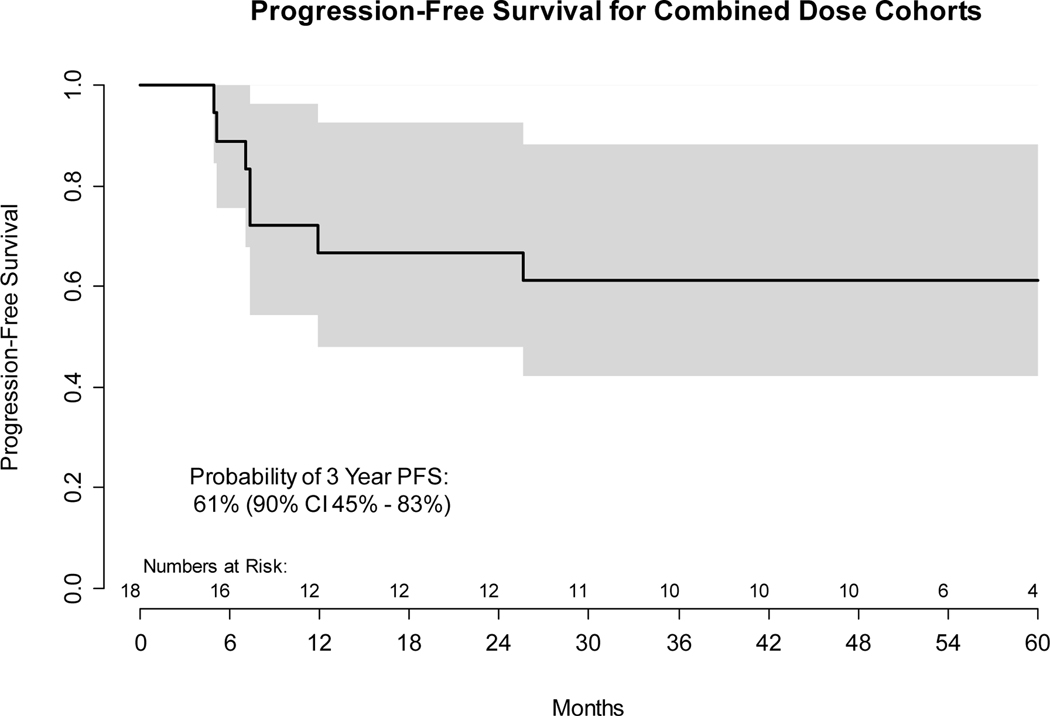
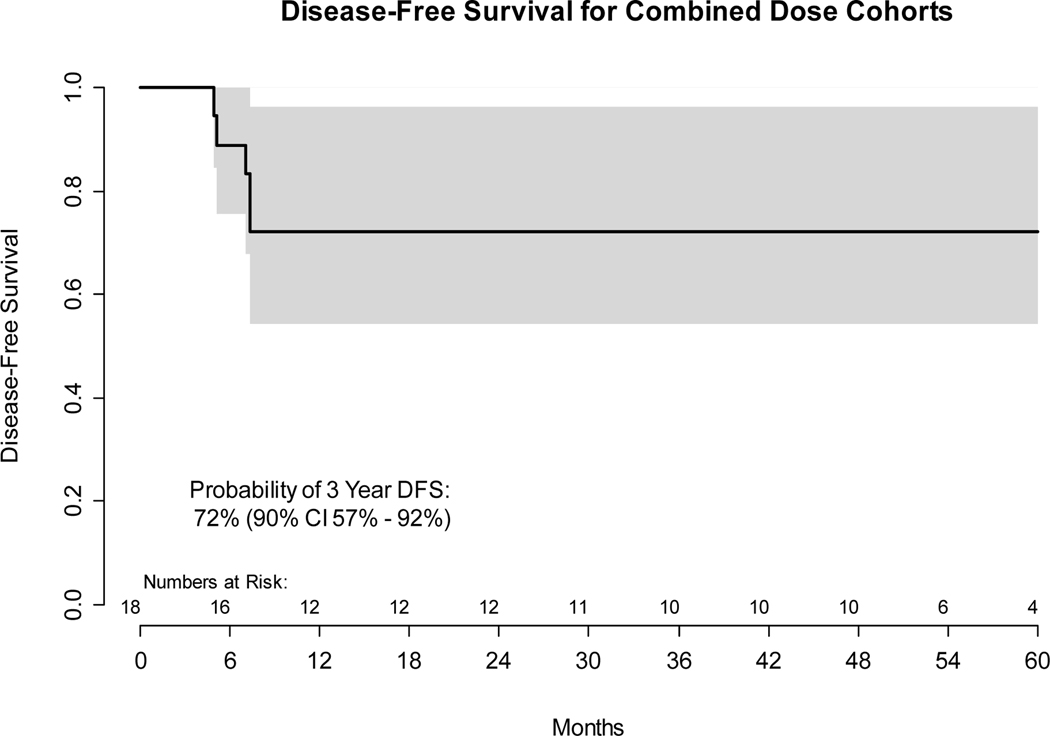
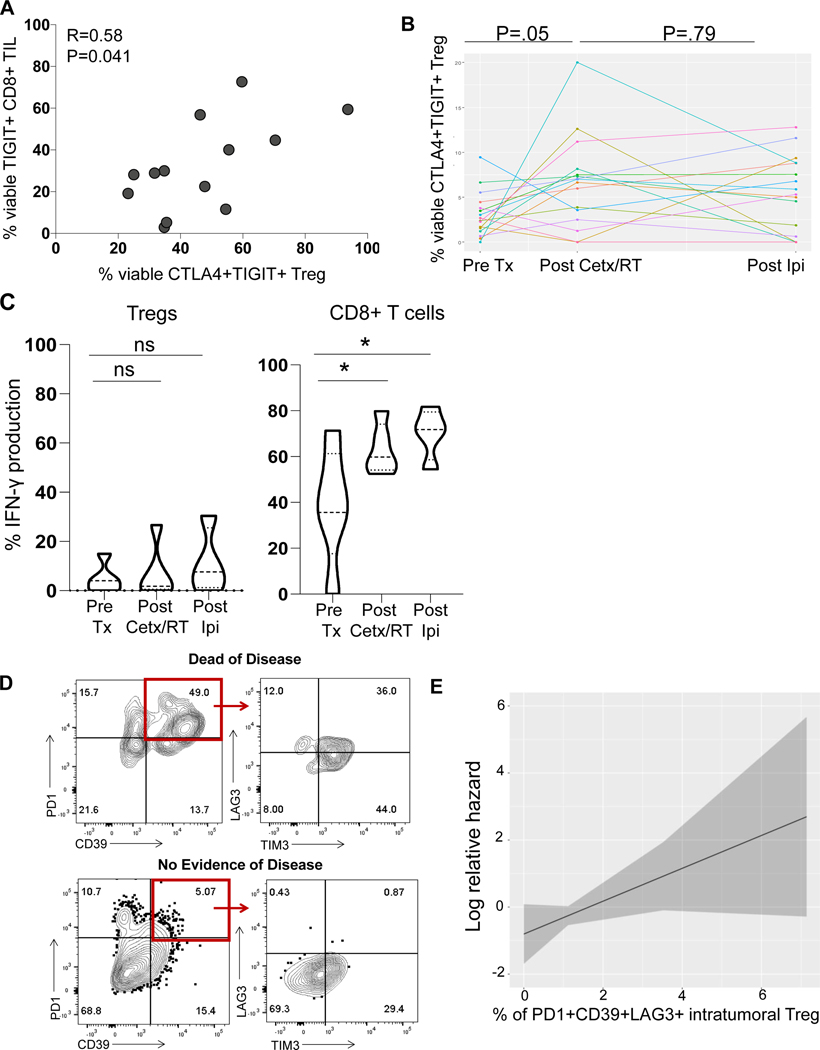
Results: From July 2013 to May 2016, 18 patients enrolled. Two of 6 in cohort 1 (ipilimumab 3 mg/kg) experienced grade 3 dermatologic DLTs, triggering deescalation of ipilimumab to 1 mg/kg. Dose level -1 was expanded to N = 12 without DLT. irAE included: grade 1, 2, and 3 dermatitis (2, 1, and 3 cases), grade 4 colitis (1), and grade 1 hyperthyroidism (1). Three-year disease-free survival (DFS) and overall survival were 72% [90% confidence interval (CI), 57-92] and 72% (90% CI, 56-92). High expression of coinhibitory receptors PD1/LAG3/CD39 on baseline tumor-infiltrating Treg was associated with worse DFS (HR = 5.6; 95% CI, 0.83-37.8; P = 0.08).
Conclusions: The RP2D for ipilimumab plus standard cetuximab-radiotherapy is 1 mg/kg in weeks 5, 8, 11, and 14. The regimen is tolerable and yields acceptable survival without cytotoxic chemotherapy.
Trial registration: ClinicalTrials.gov NCT01935921 NCT02777385.
©2022 American Association for Cancer Research.
Figures
References
-
- Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004;21:137–48. - PubMed
-
- Dunn GP, Bruce AT, Ikeda H, Old LJ, Schreiber RD. Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol 2002;3:991–8. - PubMed
-
- Vesely MD, Kershaw MH, Schreiber RD, Smyth MJ. Natural innate and adaptive immunity to cancer. Annual review of immunology 2011;29:235–71. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
