

Numerical characterization of astronaut CaOx renal stone incidence rates to quantify in-flight and post-flight relative risk
- PMID: 35091560
- PMCID: PMC8799707
- DOI: 10.1038/s41526-021-00187-z
Numerical characterization of astronaut CaOx renal stone incidence rates to quantify in-flight and post-flight relative risk
Abstract
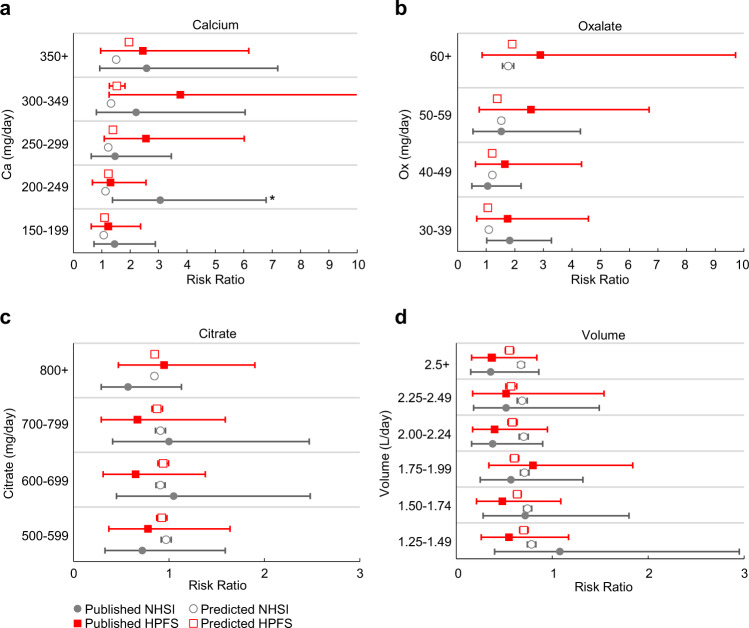
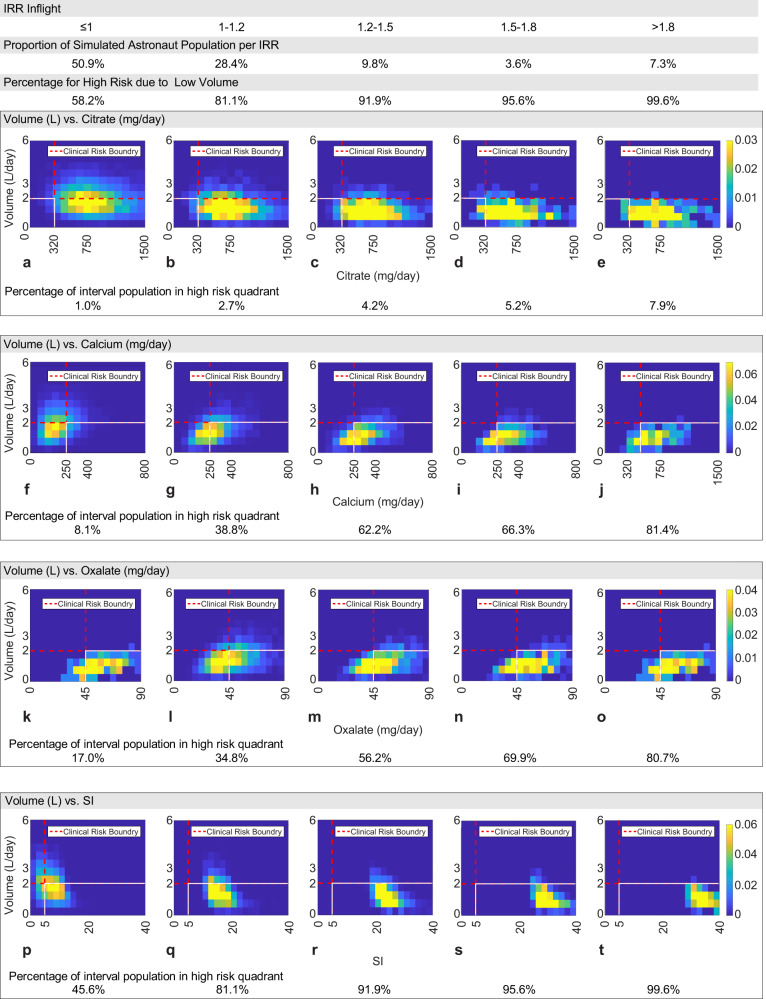
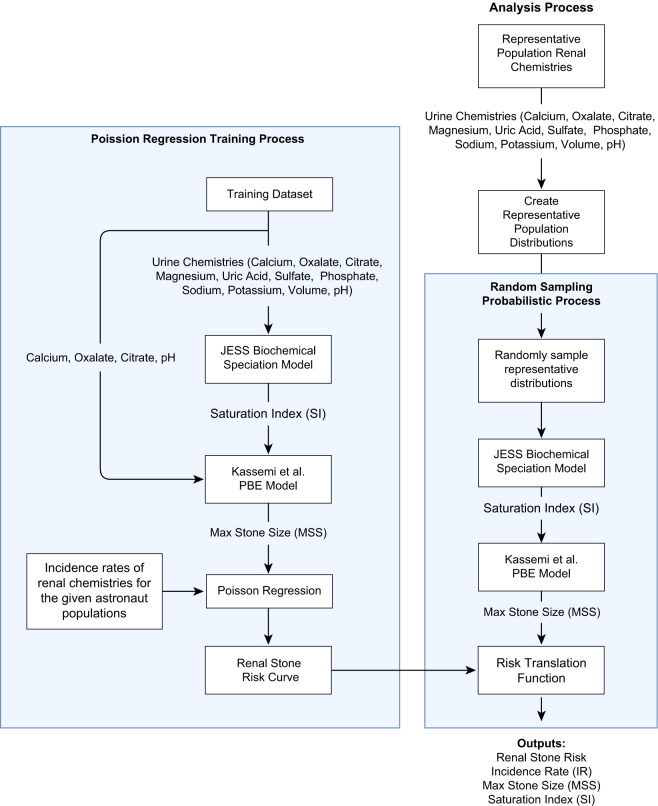
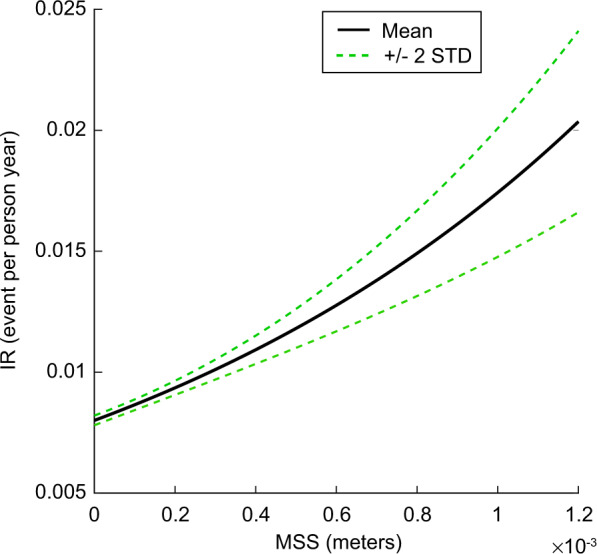
Changes in urine chemistry potentially alter the risk of renal stone formation in astronauts. Quantifying spaceflight renal stone incidence risk compared to pre-flight levels remains a significant challenge for assessing the appropriate vehicle, mission, and countermeasure design. A computational biochemistry model representing CaOx crystal precipitation, growth, and agglomeration is combined with a probabilistic analysis to predict the in- and post-flight CaOx renal stone incidence risk ratio (IRR) relative to pre-flight values using 1517 astronaut 24-h urine chemistries. Our simulations predict that in-flight fluid intake alone would need to increase from current prescriptions of 2.0-2.5 L/day to ~3.2 L/day to approach the CaOx IRR of the pre-flight population. Bone protective interventions would reduce CaOx risk to pre-flight levels if Ca excretion alone is reduced to <150 mg/day or if current levels are diminished to 190 mg/day in combination with increasing fluid intake to 2.5-2.7 L/day. This analysis provides a quantitative risk assessment that can influence the critical balance between engineering and astronaut health requirements.
© 2022. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Sibonga, J. D. & Pietrzyk, R. Evidence report: risk of renal stone formation. Evid. Rep. NASA Hum. Res. Progr. NTRS JSC-CN-39600. https://ntrs.nasa.gov/ (2017).
-
- NASA. Human Research Roadmap. https://humanresearchroadmap.nasa.gov/Evidence/ (2020).
-
- Buckey, J. C. Space Physiology (Oxford University Press, 2006).
-
- Clément, G. Fundamentals of Space Medicine (Microcosm Press, 2011).
LinkOut - more resources
Full Text Sources
