

COVID-19 CT Scan Lung Segmentation: How We Do It
- PMID: 35091874
- PMCID: PMC8796745
- DOI: 10.1007/s10278-022-00593-z
COVID-19 CT Scan Lung Segmentation: How We Do It
Abstract
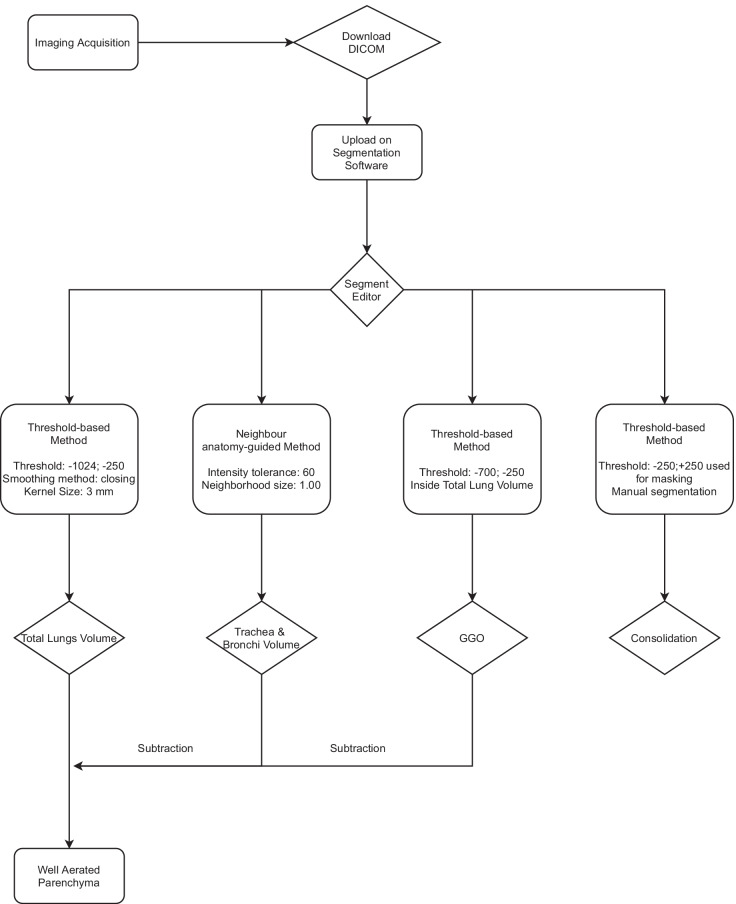
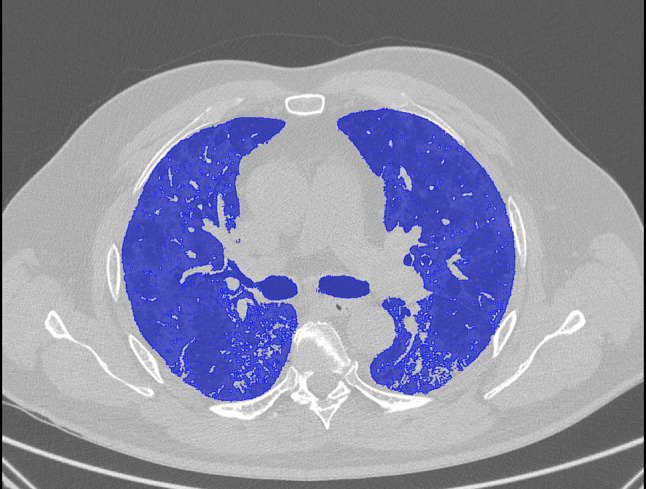
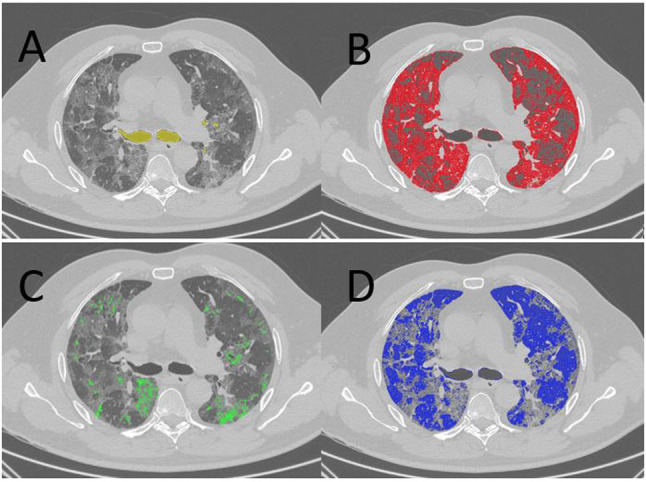
The National Health Systems have been severely stressed out by the COVID-19 pandemic because 14% of patients require hospitalization and oxygen support, and 5% require admission to an Intensive Care Unit (ICU). Relationship between COVID-19 prognosis and the extent of alterations on chest CT obtained by both visual and software-based quantification that expresses objective evaluations of the percentage of ventilated lung parenchyma compared to the affected one has been proven. While commercial applications for automatic medical image computing and visualization are expensive and limited in their spread, the open-source systems are characterized by not enough standardization and time-consuming troubles. We analyzed chest CT exams on 246 patients suspected of COVID-19 performed in the Emergency Department CT room. The lung parenchyma segmentation was obtained by a threshold-based method using the open-source 3D Slicer software and software tools called "Segment Editor" and "Segment Quantification." For the three main characteristics analyzed on lungs affected by COVID-19 pneumonia, a specifical densitometry value range was defined: from - 950 to - 700 HU for well-aerated parenchyma; from - 700 to - 250 HU for interstitial lung disease; from - 250 to 250 HU for parenchymal consolidation. For the well-aerated parenchyma and the interstitial alterations, the procedure was semi-automatic with low time consumption, whereas consolidations' analysis needed manual interventions by the operator. After the chest CT, 13% of the sample was admitted to intensive care, while 34% of them to the sub-intensive care. In patients moved to intensive care, the parenchyma analysis reported a higher crazy paving presentation. The quantitative analysis of the alterations affecting the lung parenchyma of patients with COVID-19 pneumonia can be performed by threshold method segmentation on 3D Slicer. The segmentation could have an important role in the quantification in different COVID-19 pneumonia presentations, allowing to help the clinician in the correct management of patients.
Keywords: COVID-19; Image processing, computer-assisted; Lung volume measurements; Pneumonia; Standards; Tomography, spiral computed.
© 2022. The Author(s) under exclusive licence to Society for Imaging Informatics in Medicine.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- American College of Radiology (ACR). ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 Infection. https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recom.... Published 11 Mar 2020. Accessed 1 Apr 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
