

Prevalence and Correlates of Viral Load Suppression and Human Immunodeficiency Virus (HIV) Drug Resistance Among Children and Adolescents in South Rift Valley and Kisumu, Kenya
- PMID: 35092424
- PMCID: PMC9522406
- DOI: 10.1093/cid/ciac059
Prevalence and Correlates of Viral Load Suppression and Human Immunodeficiency Virus (HIV) Drug Resistance Among Children and Adolescents in South Rift Valley and Kisumu, Kenya
Abstract
Background: Children and adolescents living with HIV (CALHIV) face unique challenges, including poorer treatment outcomes, risk for drug-resistance mutations (HIVDRMs), and limited drug formulations. We estimated viral suppression (VS) prevalence and evaluated predictors of VS and HIVDRMs in Kenya.
Methods: From 2018-2020, CALHIV 1-19 years on antiretroviral therapy (ART) >6 months were enrolled in this cross-sectional study. Participants underwent viral load (VL) testing; those with VL ≥1000 copies/mL had HIVDRM testing. Sociodemographic questionnaires and medical record abstraction were completed. VS prevalence (VL <1000 copies/mL) was estimated; robust Poisson regression models were used to estimate prevalence ratios (PRs) and 95% CIs for associations between potential predictors of VS.
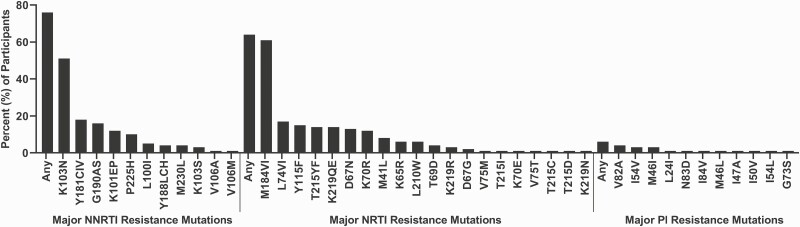
Results: Nine hundred and sixty-nine participants were enrolled. VS prevalence was .80 (95% CI: .78-.83). Being on ART >24 months (adjusted PR [aPR]: 1.22; 95% CI: 1.06-1.41), an integrase strand transfer inhibitor-containing regimen (1.13; 1.02-1.26), and attending a level 3 health facility (1.23; 1.11-1.36) were associated with VS. Missing ≥3 doses of ART in the past month (aPR: .73; 95% CI: .58-.92), having a viremic mother with HIV (.72; .53-.98), and having 3-7 (.90; .83-.97), 8-13 (.89; .82-.97), or ≥14 (.84; .77-.92) compared with <2 adherence counseling referrals were inversely associated with VS. A high proportion (n = 119, 81.5%) of unsuppressed participants had evidence of any major HIVDRM.
Conclusions: HIV treatment programs should target interventions for pediatric patients at risk for treatment failure-namely, those with a caregiver with failed VS and those struggling with adherence.
Keywords: HIV; Kenya; drug resistance; viral load.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- UNAIDS; UNICEF; World Health Organization. AIDSInfo. 2020. Available at: http://aidsinfo.unaids.org/. Accessed 3 September 2021.
-
- Bernheimer JM, Patten G, Makeleni T, et al. . Paediatric HIV treatment failure: a silent epidemic. J Int AIDS Soc 2015; 18:20090. Available at: https://pubmed.ncbi.nlm.nih.gov/26208630. - PMC - PubMed
-
- Jobanputra K, Parker LA, Azih C, et al. . Factors associated with virological failure and suppression after enhanced adherence counselling, in children, adolescents and adults on antiretroviral therapy for HIV in Swaziland. PLoS One 2015; 10:e0116144. Available at: https://pubmed.ncbi.nlm.nih.gov/25695494. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
