

Antibody Response to SARS-CoV-2 Vaccination in Patients following Allogeneic Hematopoietic Cell Transplantation
- PMID: 35092892
- PMCID: PMC8802693
- DOI: 10.1016/j.jtct.2022.01.019
Antibody Response to SARS-CoV-2 Vaccination in Patients following Allogeneic Hematopoietic Cell Transplantation
Abstract
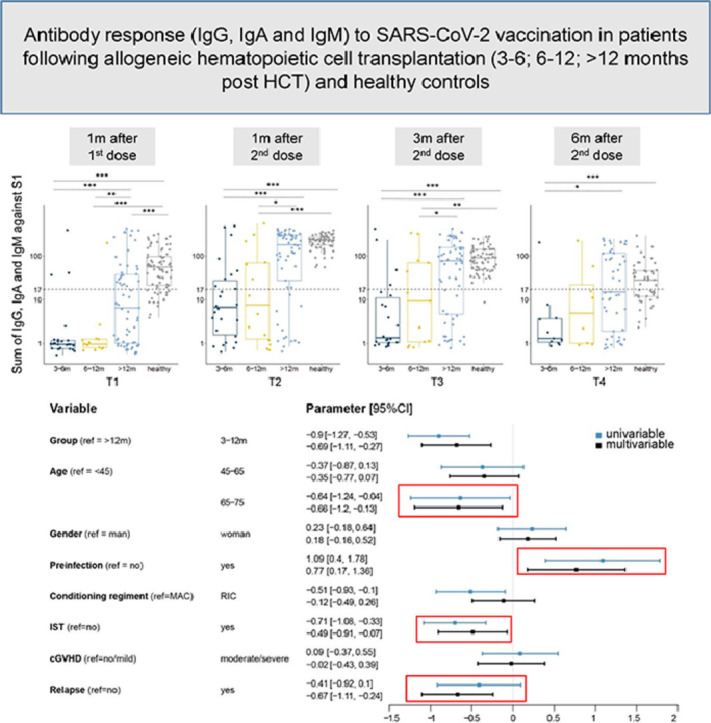
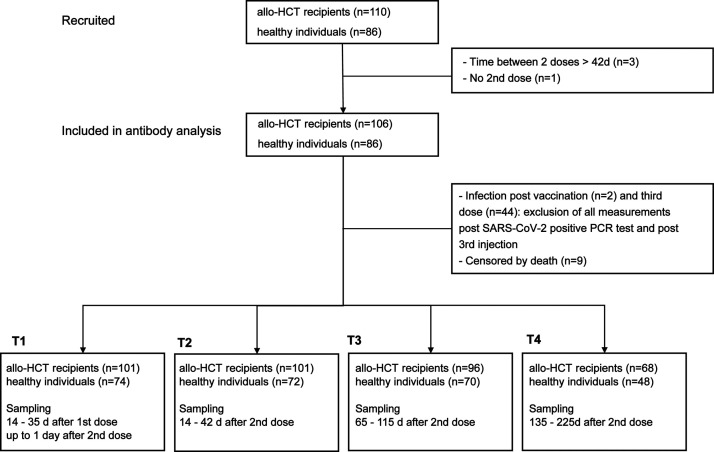
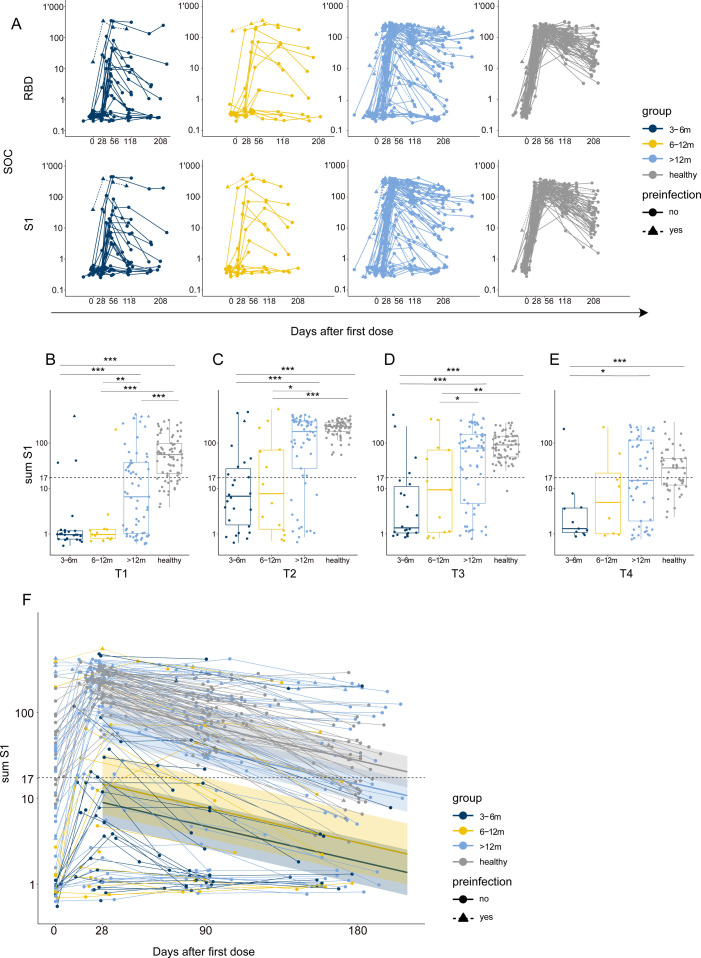
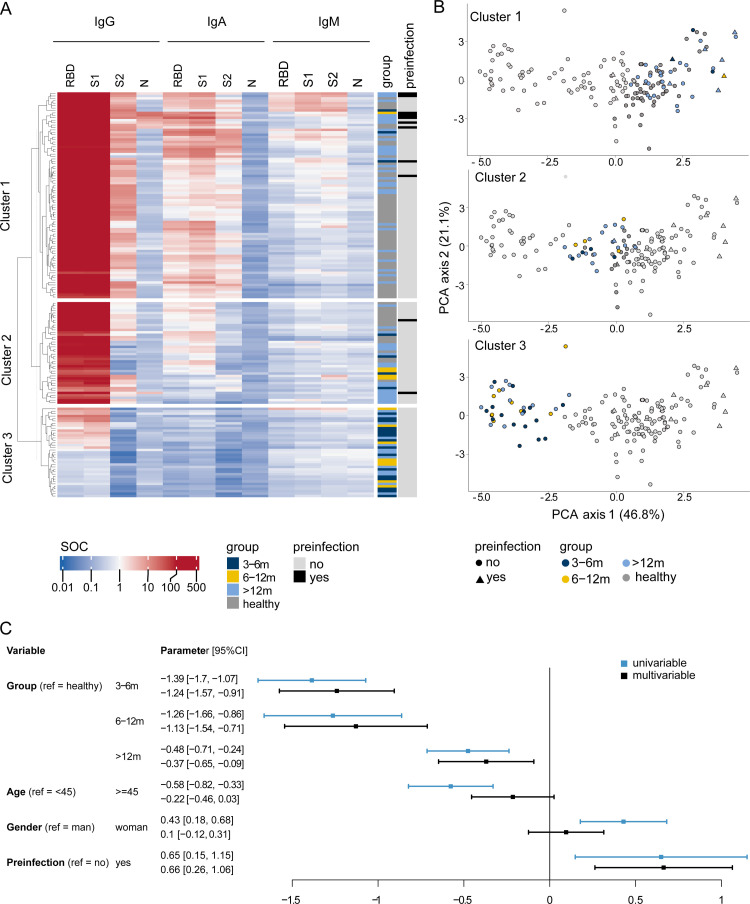
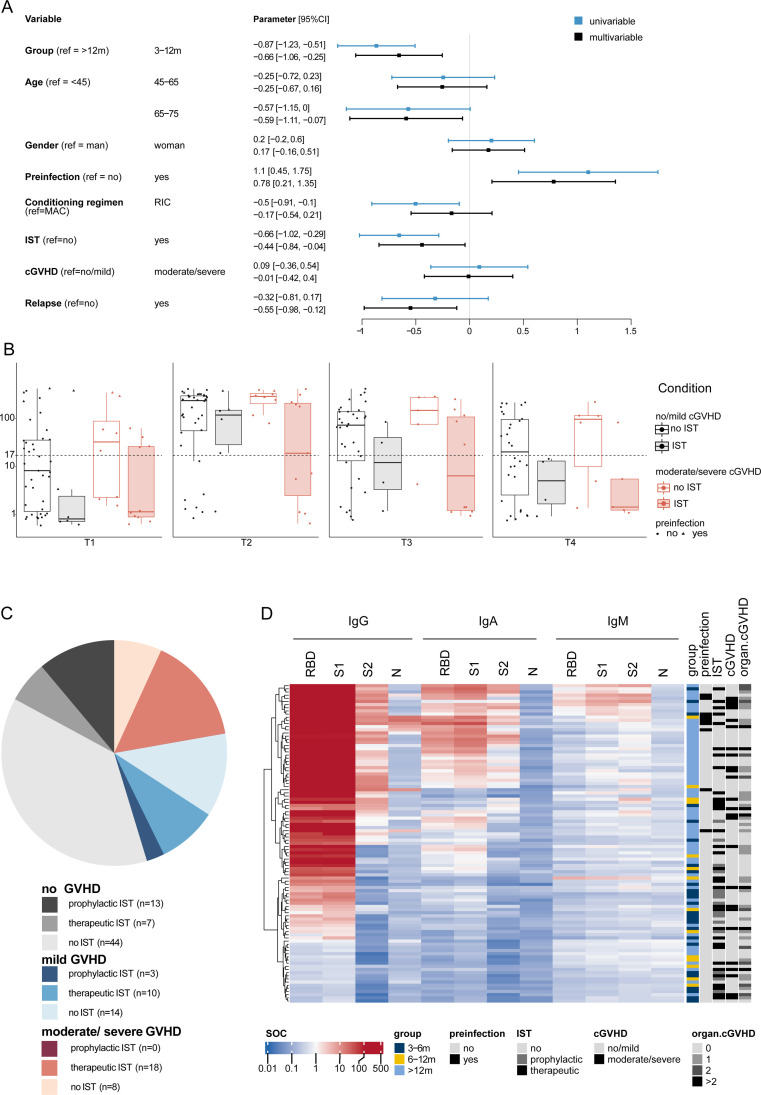
Vaccines against SARS-CoV-2 have been rapidly approved. Although pivotal studies were conducted in healthy volunteers, little information is available on the safety and efficacy of mRNA vaccines in immunocompromised patients, including recipients of allogeneic hematopoietic cell transplantation (allo-HCT). Here we used a novel assay to analyze patient- and transplantation-related factors and their influence on immune responses to SARS-CoV-2 vaccination over an extended period (up to 6 months) in a large and homogenous group of allo-HCT recipients at a single center in Switzerland. We examined longitudinal antibody responses to SARS-CoV-2 vaccination with BNT162b2 (BioNTech/Pfizer) and mRNA-1273 (Moderna) in 110 allo-HCT recipients and 86 healthy controls. Seroprofiling recording IgG, IgA, and IgM reactivity against SARS-CoV-2 antigens (receptor-binding domain, spike glycoprotein subunits S1 and S2, and nucleocapsid protein) was performed before vaccination, before the second dose, and at 1, 3, and 6 months after the second dose. Patients were stratified to 3 groups: 3 to 6 months post-allo-HCT, 6 to 12 months post-allo-HCT, and >12 months post-allo-HCT. Patients in the 3 to 6 months and 6 to 12 months post-allo-HCT groups developed significantly lower antibody titers after vaccination compared with patients in the >12 months post-allo-HCT group and healthy controls (P < .001). Within the cohort of allo-HCT recipients, patients age >65 years (P = .030), those receiving immunosuppression for prevention or treatment of graft-versus-host disease (GVHD) (P = .033), and patients with relapsed disease (P = .014) displayed low humoral immune responses to the vaccine. In contrast, the intensity of the conditioning regimen, underlying disease (myeloid/lymphoid/other), and presence of chronic GVHD had no impact on antibody levels. Antibody titers achieved the highest levels at 1 month after the second dose of the vaccine but waned substantially in all transplantation groups and healthy controls over time. This analysis of long-term vaccine antibody response is of critical importance to allo-HCT recipients and transplant physicians to guide treatment decisions regarding revaccination and social behavior during the SARS-CoV-2 pandemic.
Keywords: Allogeneic hematopoietic cell transplantation; SARS-CoV-2; Vaccination.
Copyright © 2022 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- World Health Organization. WHO coronavirus (COVID-19) dashboard. Available at: https://covid19.who.int/. Accessed November 8th 2021.
-
- Swissmedic. Swissmedic grants authorisation for the COVID-19 vaccine from Moderna. Available at: https://www.swissmedic.ch/swissmedic/en/home/humanarzneimittel/authorisa.... Accessed August 1st 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
