

Hyperimmune immunoglobulin for hospitalised patients with COVID-19 (ITAC): a double-blind, placebo-controlled, phase 3, randomised trial
- PMID: 35093205
- PMCID: PMC8797010
- DOI: 10.1016/S0140-6736(22)00101-5
Hyperimmune immunoglobulin for hospitalised patients with COVID-19 (ITAC): a double-blind, placebo-controlled, phase 3, randomised trial
Abstract
Background: Passive immunotherapy using hyperimmune intravenous immunoglobulin (hIVIG) to SARS-CoV-2, derived from recovered donors, is a potential rapidly available, specific therapy for an outbreak infection such as SARS-CoV-2. Findings from randomised clinical trials of hIVIG for the treatment of COVID-19 are limited.
Methods: In this international randomised, double-blind, placebo-controlled trial, hospitalised patients with COVID-19 who had been symptomatic for up to 12 days and did not have acute end-organ failure were randomly assigned (1:1) to receive either hIVIG or an equivalent volume of saline as placebo, in addition to remdesivir, when not contraindicated, and other standard clinical care. Randomisation was stratified by site pharmacy; schedules were prepared using a mass-weighted urn design. Infusions were prepared and masked by trial pharmacists; all other investigators, research staff, and trial participants were masked to group allocation. Follow-up was for 28 days. The primary outcome was measured at day 7 by a seven-category ordinal endpoint that considered pulmonary status and extrapulmonary complications and ranged from no limiting symptoms to death. Deaths and adverse events, including organ failure and serious infections, were used to define composite safety outcomes at days 7 and 28. Prespecified subgroup analyses were carried out for efficacy and safety outcomes by duration of symptoms, the presence of anti-spike neutralising antibodies, and other baseline factors. Analyses were done on a modified intention-to-treat (mITT) population, which included all randomly assigned participants who met eligibility criteria and received all or part of the assigned study product infusion. This study is registered with ClinicalTrials.gov, NCT04546581.
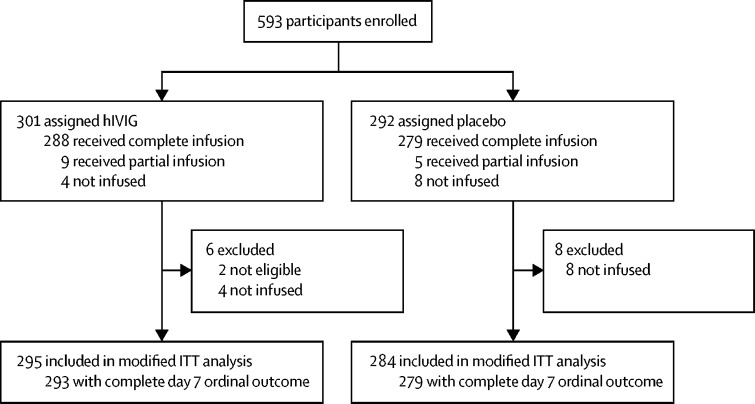
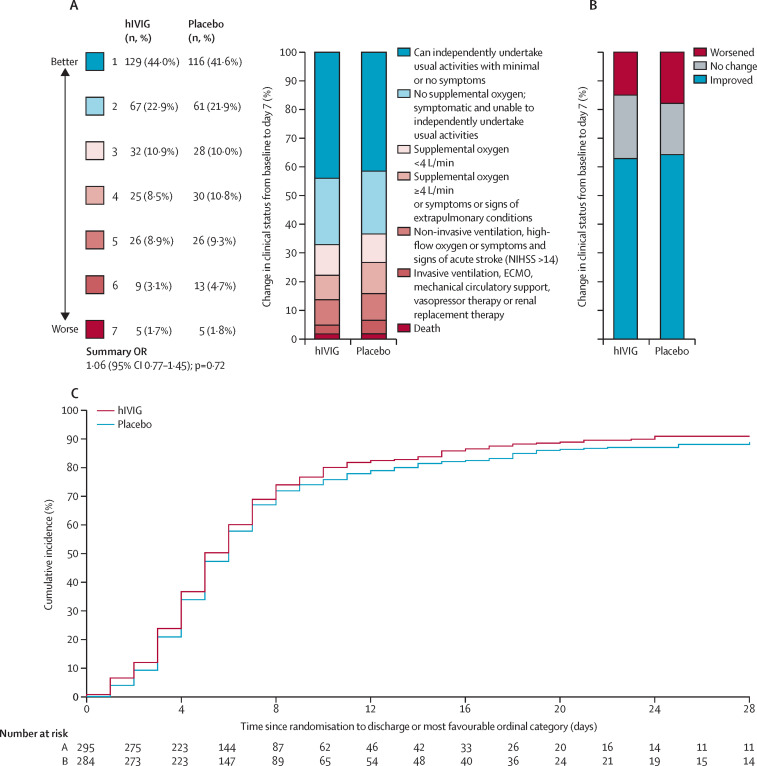
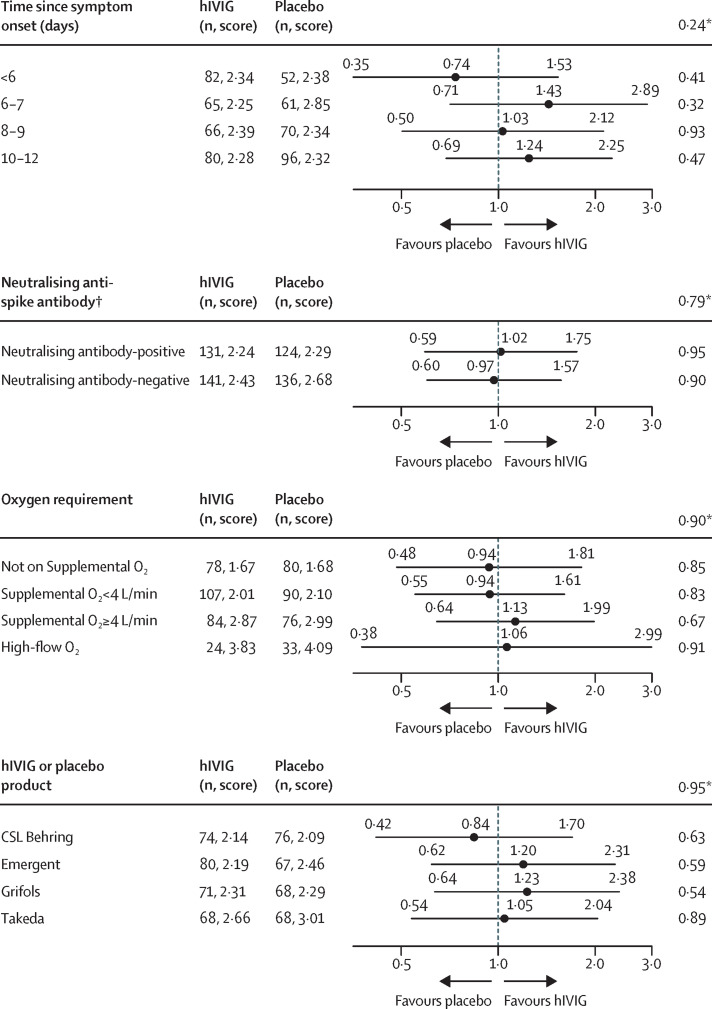
Findings: From Oct 8, 2020, to Feb 10, 2021, 593 participants (n=301 hIVIG, n=292 placebo) were enrolled at 63 sites in 11 countries; 579 patients were included in the mITT analysis. Compared with placebo, the hIVIG group did not have significantly greater odds of a more favourable outcome at day 7; the adjusted OR was 1·06 (95% CI 0·77-1·45; p=0·72). Infusions were well tolerated, although infusion reactions were more common in the hIVIG group (18·6% vs 9·5% for placebo; p=0·002). The percentage with the composite safety outcome at day 7 was similar for the hIVIG (24%) and placebo groups (25%; OR 0·98, 95% CI 0·66-1·46; p=0·91). The ORs for the day 7 ordinal outcome did not vary for subgroups considered, but there was evidence of heterogeneity of the treatment effect for the day 7 composite safety outcome: risk was greater for hIVIG compared with placebo for patients who were antibody positive (OR 2·21, 95% CI 1·14-4·29); for patients who were antibody negative, the OR was 0·51 (0·29-0·90; pinteraction=0·001).
Interpretation: When administered with standard of care including remdesivir, SARS-CoV-2 hIVIG did not demonstrate efficacy among patients hospitalised with COVID-19 without end-organ failure. The safety of hIVIG might vary by the presence of endogenous neutralising antibodies at entry.
Funding: US National Institutes of Health.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests MNP reports grants from University of Minnesota (Minneapolis, MN, USA) during the conduct of the study, grants from National Institutes of Health (NIH) during the conduct of the study, Gilead Sciences, ViiV, Celgene, and Janssen Pharmaceuticals outside the submitted work. AGB reports grants from University of Minnesota during the conduct of the study, grants from UK Research and Innovation (UKRI) outside of the submitted work. MKJ reports donation of trial medications from Regeneron Pharmaceuticals, Janssen Pharmaceuticals, and from Merck; and grants, personal fees, and donation of trial medications from Gilead Sciences, outside the submitted work. SLP reports grants from University of Minnesota during the conduct of the study, European and Developing Countries Clinical Trials Partnership, UKRI, Academy of Medical Sciences, ViiV Healthcare, Medical Research Council, and Gilead Sciences outside the submitted work. MKD reports being an employee of CSL Behring. SP reports being an employee of CSL Behring. CH reports being an employee of Emergent; Ramanathan reports being an employee of Emergent. HC reports being an employee of Gilead Sciences. EM reports being an employee of Grifols. TW reports being an employee of Grifols. JVT reports being an employee of Takeda. LY reports being an employee of Takeda. JDN reports grants from NIH during the conduct of the study. All other members of the writing group declare no competing interests.
Figures
References
-
- Horby PW, Pessoa-Amorim G, Peto L, et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): preliminary results of a randomised, controlled, open-label, platform trial. Lancet. 2021;97:637–645.
-
- Long QX, Liu BZ, Deng HJ, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nat Med. 2020;26:845–848. - PubMed
