

Distinguishing Multisystem Inflammatory Syndrome in Children From COVID-19, Kawasaki Disease and Toxic Shock Syndrome
- PMID: 35093995
- PMCID: PMC8919949
- DOI: 10.1097/INF.0000000000003449
Distinguishing Multisystem Inflammatory Syndrome in Children From COVID-19, Kawasaki Disease and Toxic Shock Syndrome
Abstract
Background: Distinguishing multisystem inflammatory syndrome in children (MIS-C) from coronavirus disease 2019 (COVID-19), Kawasaki disease (KD), and toxic shock syndrome (TSS) can be challenging. Because clinical management of these conditions can vary, timely and accurate diagnosis is essential.
Methods: Data were collected from patients <21 years of age hospitalized with MIS-C, COVID-19, KD, and TSS in 4 major health care institutions. Patient demographics and clinical and laboratory data were compared among the 4 conditions, and a diagnostic scoring tool was developed to assist in clinical diagnosis.
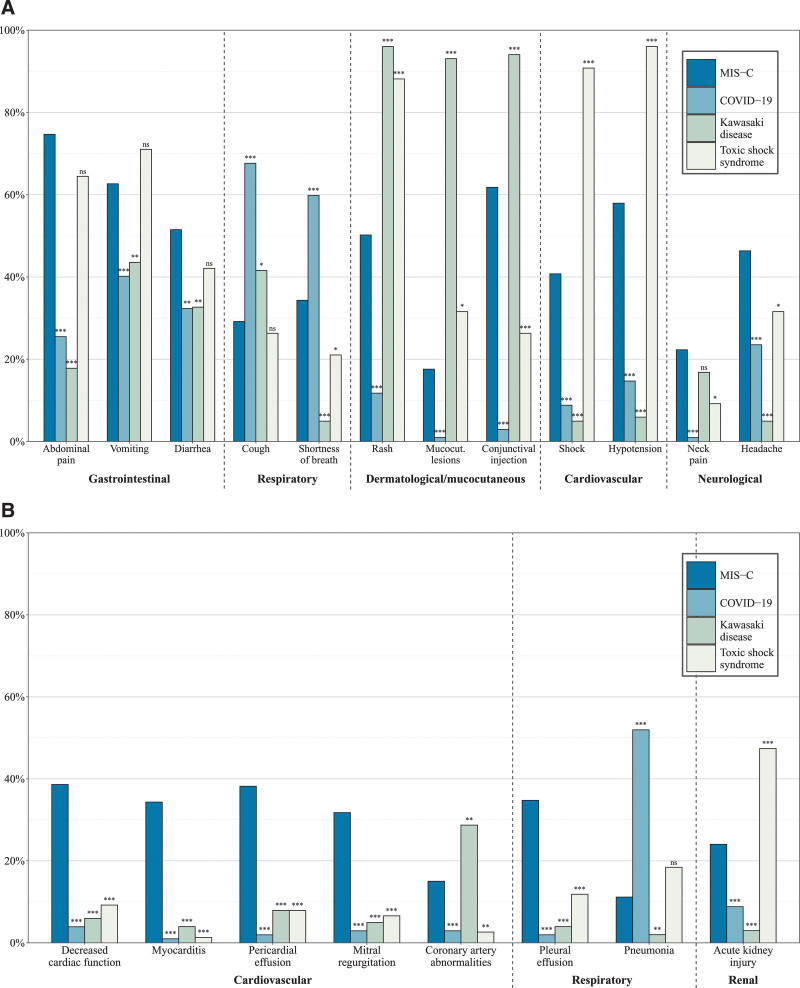
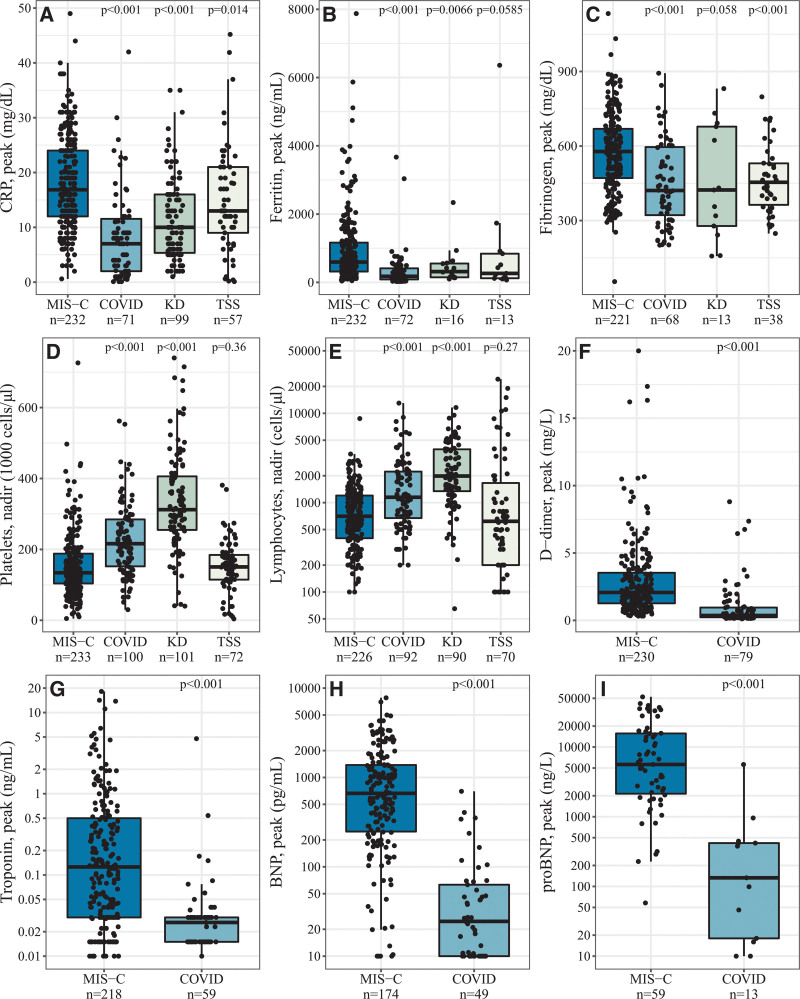
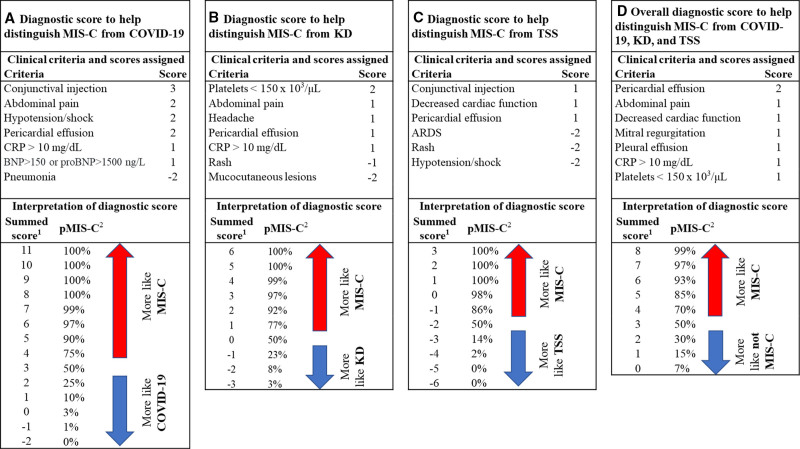
Results: A total of 233 patients with MIS-C, 102 with COVID-19, 101 with KD, and 76 with TSS were included in the analysis. Patients with MIS-C had the highest prevalence of decreased cardiac function (38.6%), myocarditis (34.3%), pericardial effusion (38.2%), mitral regurgitation (31.8%) and pleural effusion (34.8%) compared with patients with the other conditions. Patients with MIS-C had increased peak levels of C-reactive protein and decreased platelets and lymphocyte nadir counts compared with patients with COVID-19 and KD and elevated levels of troponin, brain natriuretic peptide and pro-brain natriuretic peptide compared with COVID-19. Diagnostic scores utilizing clinical findings effectively distinguished MIS-C from COVID-19, KD, and TSS, with internal validation showing area under the curve ranging from 0.87 to 0.97.
Conclusions: Compared with COVID-19, KD, and TSS, patients with MIS-C had significantly higher prevalence of cardiac complications, elevated markers of inflammation and cardiac damage, thrombocytopenia, and lymphopenia. Diagnostic scores can be a useful tool for distinguishing MIS-C from COVID-19, KD, and TSS.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Figures
References
-
- Dufort EM, Koumans EH, Chow EJ, et al. New York State and Centers for Disease Control and Prevention Multisystem Inflammatory Syndrome in Children Investigation Team . New York State and Centers for Disease Control and Prevention Multisystem Inflammatory Syndrome in Children Investigation Team Multisystem inflammatory syndrome in children in New York State. N Engl J Med. 2020;383:347–358. - PMC - PubMed
-
- The Royal College of Paediatrics and Child Health. Guidance: paediatric multisystem inflammatory syndrome temporally associated with COVID-19. Available at: https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-.... Accessed December 16, 2020. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
