

Endotheliopathy is associated with slower liberation from mechanical ventilation: a cohort study
- PMID: 35094711
- PMCID: PMC8801241
- DOI: 10.1186/s13054-021-03877-y
Endotheliopathy is associated with slower liberation from mechanical ventilation: a cohort study
Abstract
Background: Endotheliopathy is suggested as pivotal pathophysiology of sepsis and trauma-associated organ failure, but its role in acute respiratory failure is not yet determined. We investigated if endotheliopathy biomarkers at ICU admission are associated with illness severity and clinical outcomes in patients with acute respiratory failure requiring mechanical ventilation.
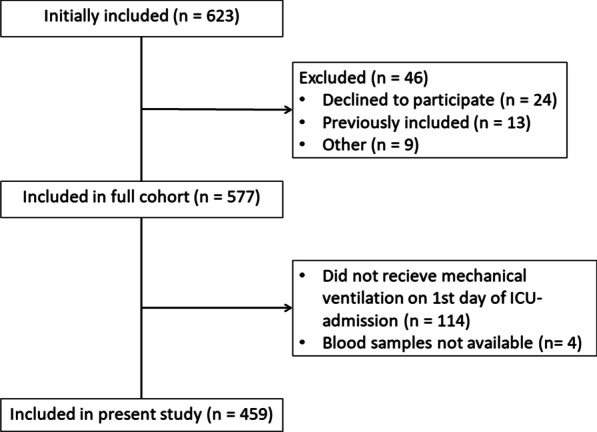
Methods: We conducted a prospective single-center cohort study including 459 mechanically ventilated adults at ICU admission. Plasma levels of three endotheliopathy biomarkers were measured at ICU admission: Syndecan-1, soluble Thrombomodulin (sTM), and Platelet Endothelial Cell Adhesion Molecule-1 (PECAM-1). The primary outcome was the rate of liberation from mechanical ventilation, which is presented together with the rate of the competing risk of death while still on mechanical ventilation. Secondary outcomes were PaO2/FiO2-ratios on admission and on last measurement in patients dying within five days, and 30-day all-cause mortality. The primary outcome and 30-day all-cause mortality were analyzed using Cox regression, controlled for gender, age, chronic obstructive pulmonary disease, septic shock, heart failure, PaO2/FiO2-ratio at admission, respiratory infection, acute kidney injury, and bilirubin. PaO2/FiO2-ratios were analyzed using linear regression, controlled for age, chronic obstructive pulmonary disease, respiratory infection, and shock.
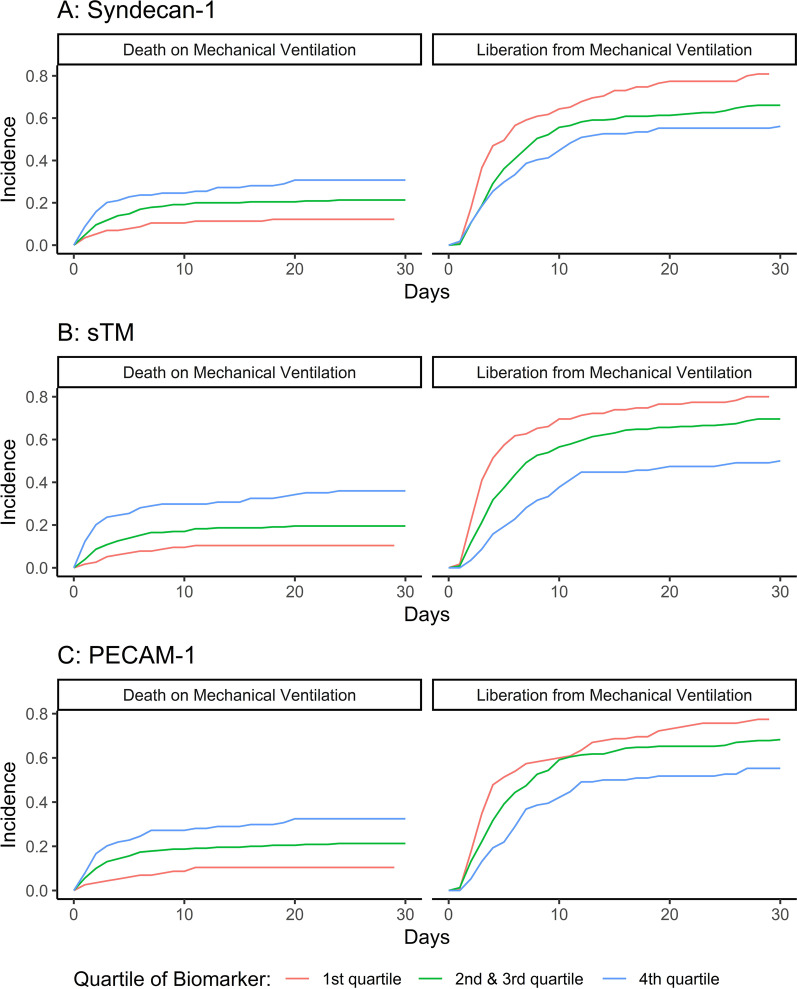
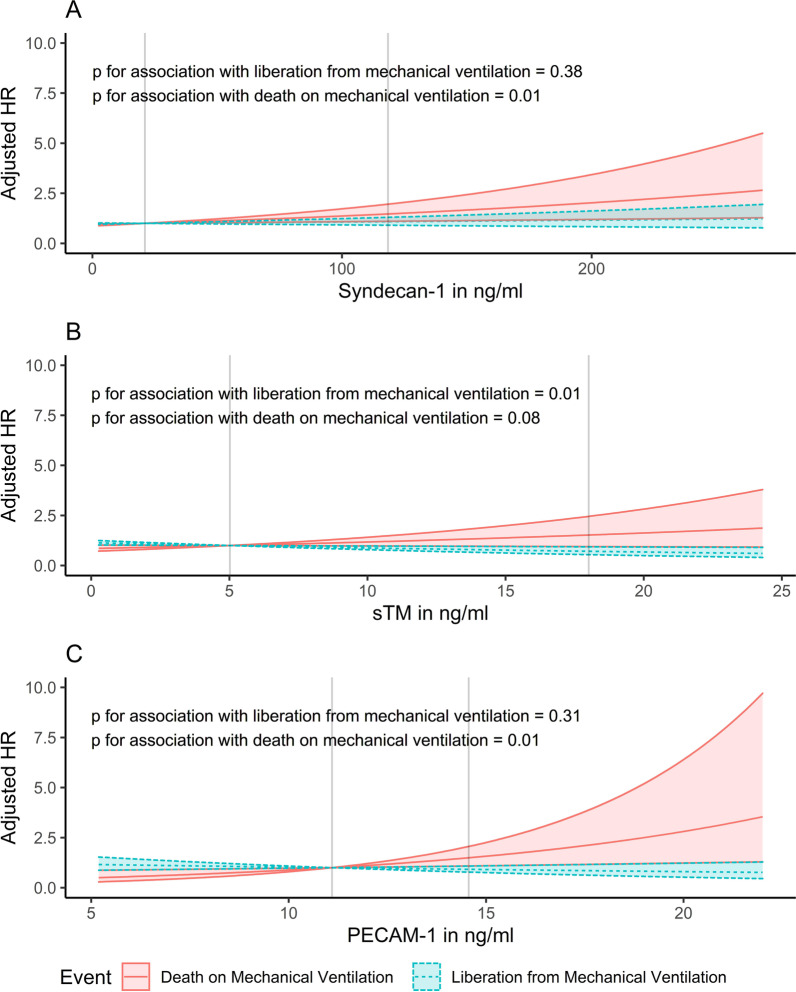
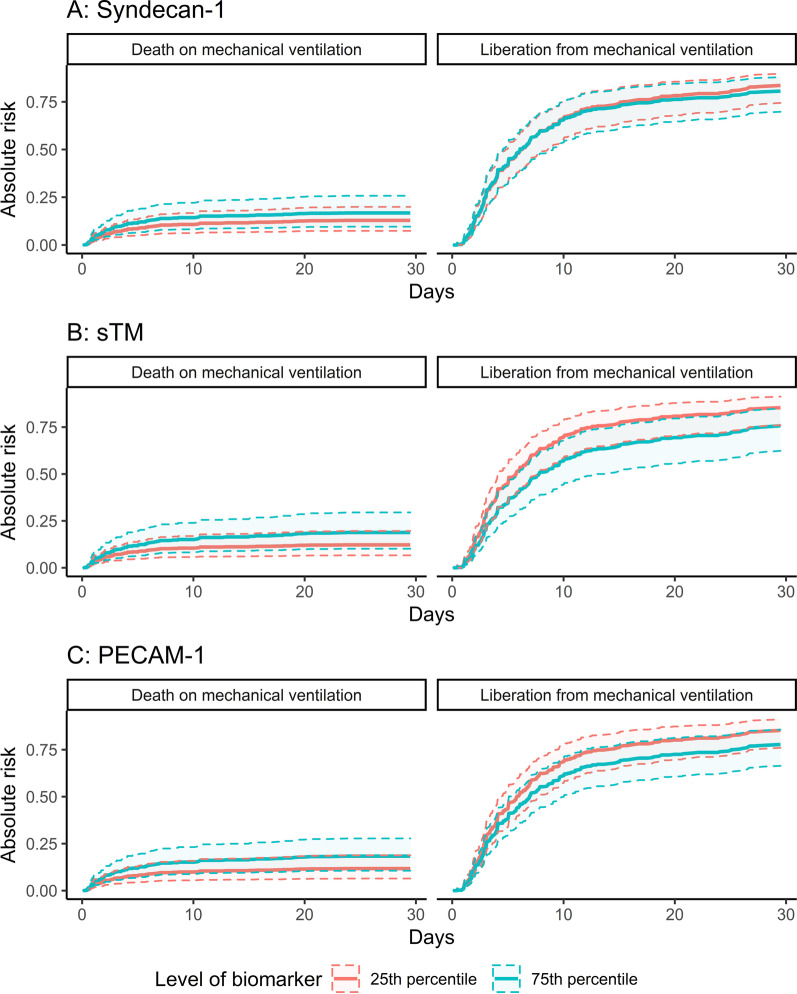
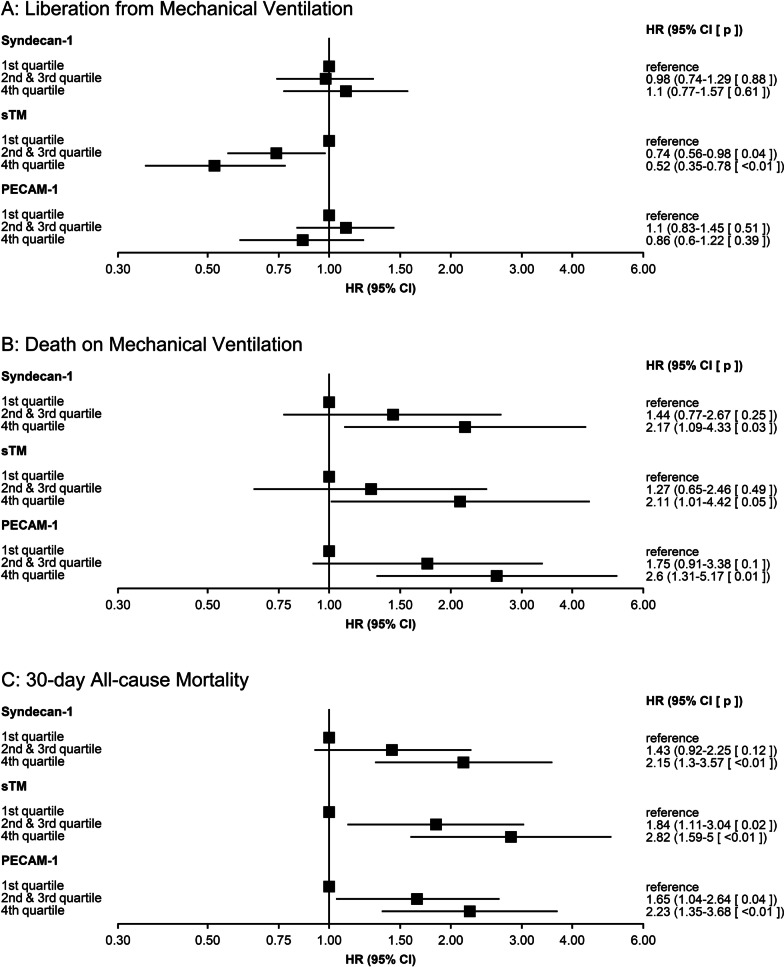
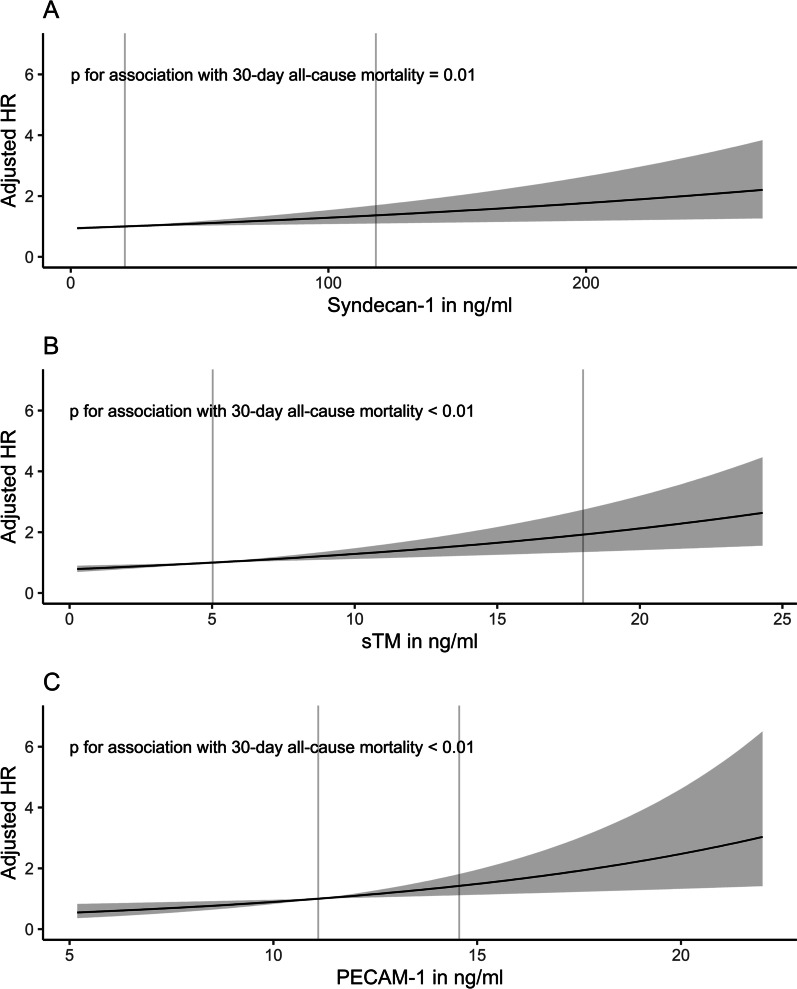
Results: Patients with high sTM were liberated from mechanical ventilation at a lower rate (adjusted hazard ratio (HR) 0.71, for an increase from the 25th to the 75th percentile, 95% confidence interval (CI) 0.54-0.93, p = 0.01). Patients with high PECAM-1 were liberated from mechanical ventilation at a lower rate, but only during the first 5 days (adjusted HR 0.72, for an increase from the 25th to the 75th percentile, 95% CI 0.58-0.9, p < 0.01). High levels of Syndecan-1 and PECAM-1 were associated with a higher rate of death while still on mechanical ventilation. sTM and PECAM-1 were negatively associated with PaO2/FiO2-ratio at ICU admission and no biomarker was associated with last measured PaO2/FiO2-ratio. High levels of all biomarkers were associated with higher 30-day all-cause mortality.
Conclusion: In acute respiratory failure, endotheliopathy biomarkers are associated with lower rates of liberation from mechanical ventilation, hypoxemia at ICU admission, and 30-day all-cause mortality.
Keywords: Endothelium; Observational study; Platelet Endothelial Cell Adhesion Molecule-1; Respiratory insufficiency/physiopathology; Syndecan-1; Thrombomodulin; Vascular.
© 2022. The Author(s).
Conflict of interest statement
No authors have any conflicts of interests to declare.
Figures
Similar articles
-
Novel subgroups in acute respiratory failure based on the trajectories of three endotheliopathy biomarkers: A cohort study.Acta Anaesthesiol Scand. 2023 Aug;67(7):896-908. doi: 10.1111/aas.14246. Epub 2023 Apr 12. Acta Anaesthesiol Scand. 2023. PMID: 37042167
-
The evolution of the ventilatory ratio is a prognostic factor in mechanically ventilated COVID-19 ARDS patients.Crit Care. 2021 Sep 13;25(1):331. doi: 10.1186/s13054-021-03727-x. Crit Care. 2021. PMID: 34517881 Free PMC article.
-
Clinical characteristics and outcomes of invasively ventilated patients with COVID-19 in Argentina (SATICOVID): a prospective, multicentre cohort study.Lancet Respir Med. 2021 Sep;9(9):989-998. doi: 10.1016/S2213-2600(21)00229-0. Epub 2021 Jul 2. Lancet Respir Med. 2021. PMID: 34224674 Free PMC article.
-
Management strategies and outcomes predictors of interstitial lung disease exacerbation admitted to an intensive care setting: A narrative review.J Crit Care Med (Targu Mures). 2025 Apr 30;11(2):112-121. doi: 10.2478/jccm-2025-0013. eCollection 2025 Apr. J Crit Care Med (Targu Mures). 2025. PMID: 40386698 Free PMC article. Review.
-
Target arterial PO2 according to the underlying pathology: a mini-review of the available data in mechanically ventilated patients.Ann Intensive Care. 2021 Jun 2;11(1):88. doi: 10.1186/s13613-021-00872-y. Ann Intensive Care. 2021. PMID: 34076802 Free PMC article. Review.
Cited by
-
The Association Between Dysglycemia and Endotheliopathy in ICU Patients With and Without Diabetes: A Cohort Study.Crit Care Explor. 2025 Mar 24;7(4):e1229. doi: 10.1097/CCE.0000000000001229. eCollection 2025 Apr 1. Crit Care Explor. 2025. PMID: 40126923 Free PMC article.
-
Efficacy and safety of a 72-h infusion of prostacyclin (1 ng/kg/min) in mechanically ventilated patients with pulmonary infection and endotheliopathy-protocol for the multicenter randomized, placebo-controlled, blinded, investigator-initiated COMBAT-ARF trial.Acta Anaesthesiol Scand. 2025 Jan;69(1):e14565. doi: 10.1111/aas.14565. Acta Anaesthesiol Scand. 2025. PMID: 39704260 Free PMC article.
-
Nonlinear relationship between platelet count and 30-day in-hospital mortality in ICU acute respiratory failure patients: a multicenter retrospective cohort study.Eur J Med Res. 2024 Jun 8;29(1):312. doi: 10.1186/s40001-024-01909-1. Eur J Med Res. 2024. PMID: 38849948 Free PMC article.
-
Changes in nitric oxide inhibitors and mortality in critically ill patients: a cohort study.Ann Intensive Care. 2024 Aug 27;14(1):133. doi: 10.1186/s13613-024-01362-7. Ann Intensive Care. 2024. PMID: 39190083 Free PMC article.
-
Bacterial lipopolysaccharide-induced endothelial activation and dysfunction: a new predictive and therapeutic paradigm for sepsis.Eur J Med Res. 2023 Sep 12;28(1):339. doi: 10.1186/s40001-023-01301-5. Eur J Med Res. 2023. PMID: 37700349 Free PMC article. Review.
References
-
- Zambon M, Vincent JL. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest Am Coll Chest Phys. 2008;133:1120–1127. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
