

Maternal selection of human embryos in early gestation: Insights from recurrent miscarriage
- PMID: 35094946
- PMCID: PMC9325922
- DOI: 10.1016/j.semcdb.2022.01.007
Maternal selection of human embryos in early gestation: Insights from recurrent miscarriage
Abstract
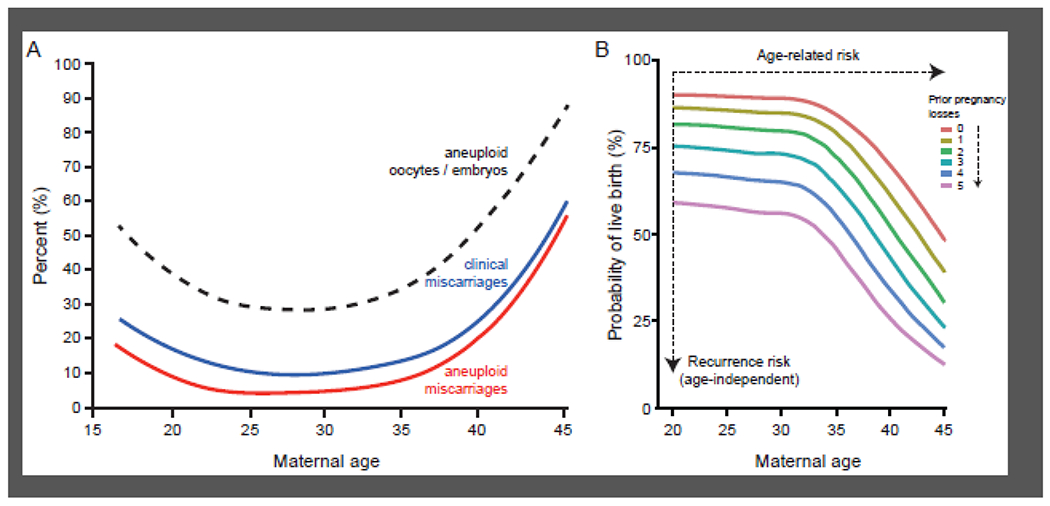
Compared to most mammals, human pregnancy is unusual in that it involves chromosomally diverse embryos, cyclical breakdown and regeneration of the uterine mucosa, and intimate integration of fetal and maternal cells at the uteroplacental interface. Not surprisingly, pregnancy often falters in early gestation. Whether these losses result in clinical miscarriages depends on the origins and impacts of chromosomal errors on fetal development and the ability of the decidualizing endometrium to engage in embryo biosensing and selection. Aneuploidy originating in oocytes during meiosis drives the age-related risk of miscarriage. By contrast, the frequency of endometrial cycles with an impaired decidual response may account for the stepwise increase in miscarriage rates with each pregnancy loss independently of maternal age. Additional physiological mechanisms operate in early gestation to ensure that most failing pregnancies are lost before vascular maternal-fetal connections are established by the end of the first trimester. Here, we summarise how investigations into the mechanisms that cause miscarriage led to new insights into the processes that govern maternal selection of human embryos in early gestation.
Keywords: Aneuploidy; Decidualization; Embryo; Endometrium; Miscarriage; Placenta; Selection.
Copyright © 2022. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest None.
Figures


References
-
- Zinaman MJ, Clegg ED, Brown CC, O’Connor J, Selevan SG, Estimates of human fertility and pregnancy loss, Fertility and sterility 65(3) (1996): 503–9. - PubMed
-
- Quenby S, Gallos ID, Dhillon-Smith RK, Podesek M, Stephenson MD, Fisher J, Brosens JJ, Brewin J, Ramhorst R, Lucas ES, McCoy RC, Anderson R, Daher S, Regan L, Al-Memar M, Bourne T, MacIntyre DA, Rai R, Christiansen OB, Sugiura-Ogasawara M, Odendaal J, Devall AJ, Bennett PR, Petrou S, Coomarasamy A, Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss, Lancet 397(10285) (2021): 1658–1667, 10.1016/S0140-6736(21)00682-6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
