

Effect of Theta Burst Stimulation-Patterned rTMS on Motor and Nonmotor Dysfunction of Parkinson's Disease: A Systematic Review and Metaanalysis
- PMID: 35095722
- PMCID: PMC8790062
- DOI: 10.3389/fneur.2021.762100
Effect of Theta Burst Stimulation-Patterned rTMS on Motor and Nonmotor Dysfunction of Parkinson's Disease: A Systematic Review and Metaanalysis
Abstract
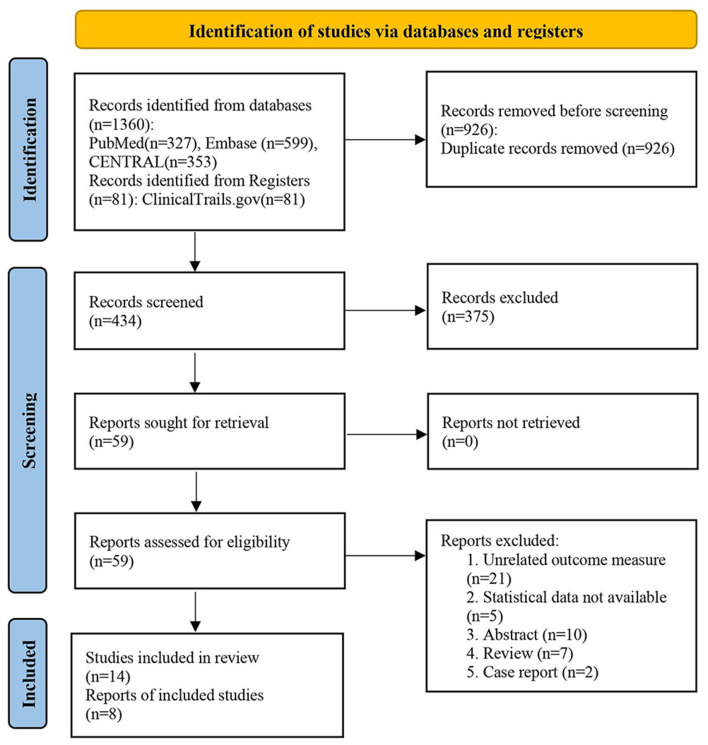
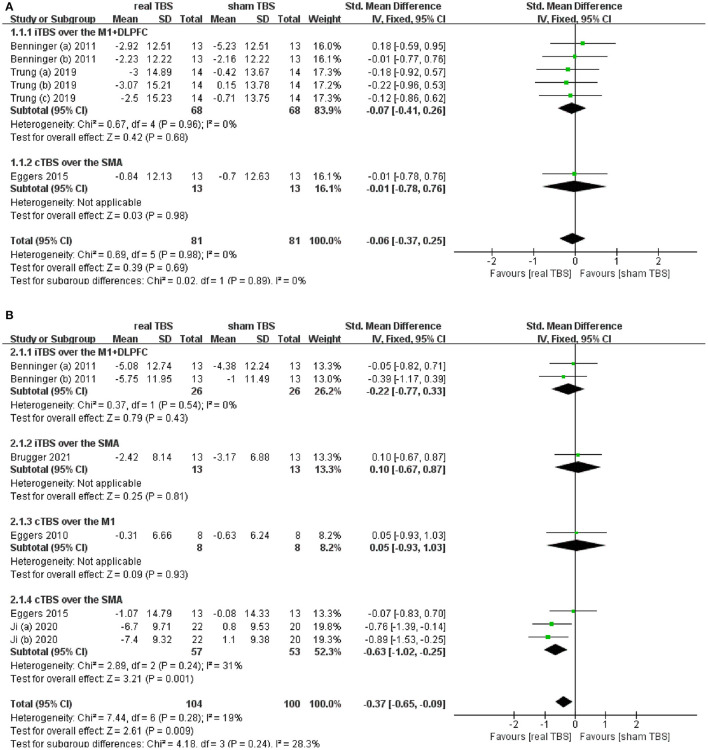
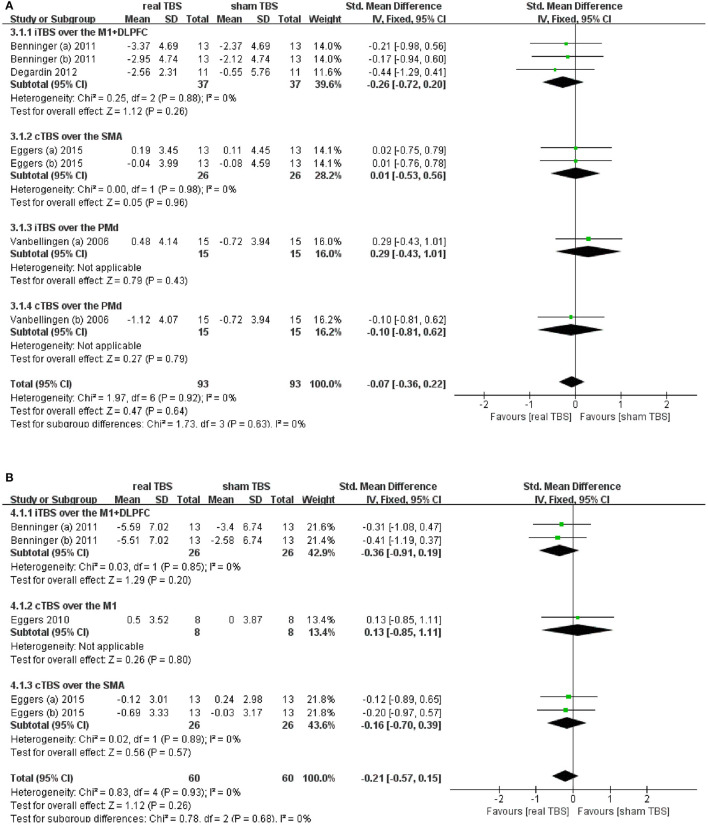
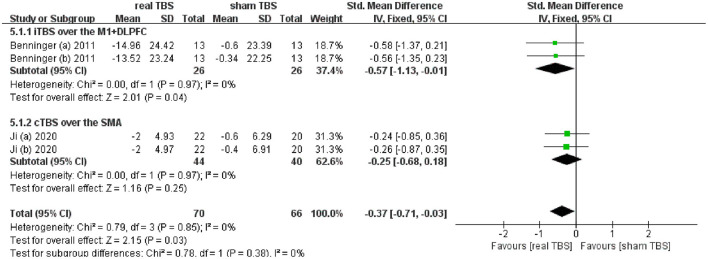
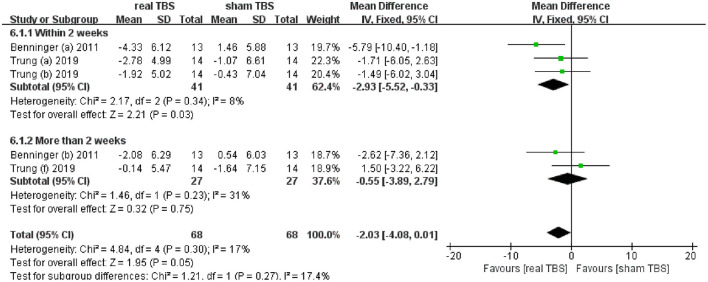
Background: Theta burst stimulation (TBS), a type of patterned repetitive transcranial magnetic stimulation (rTMS), has several advantages, such as short time of single treatment and low stimulation intensity compared with traditional rTMS. Since the efficacy of TBS on the symptoms of Parkinson's disease (PD) was inconsistent among different studies, we systematically searched these studies and quantitatively analyzed the therapeutic effect of TBS for patients with PD. Methods: We followed the recommended PRISMA guidelines for systematic reviews. Studies from PubMed, EMBASE, CENTRAL, and ClinicalTrials.gov from January 1, 2005 of each database to September 30, 2021 were analyzed. We also manually retrieved studies of reference. Results: Eight eligible studies with 189 participants (received real TBS and/or sham TBS) were included. This metaanalysis found that TBS did not significantly improve Unified Parkinson's Disease Rating Scale part III (UPDRS-III) score in the "on" medicine state (SMD = -0.06; 95% CI, -0.37 to 0.25; p = 0.69; I 2 = 0%), while, it brought significant improvement of UPDRS-III scores in the "off" medicine state (SMD = -0.37; 95% CI, -0.65 to -0.09; p < 0.01; I 2 = 19%). Subgroup analysis found that merely continuous TBS (cTBS) over the supplementary motor area (SMA) brought significant improvement of UPDRS-III score (SMD = -0.63; 95% CI, -1.02 to -0.25; p < 0.01). TBS had insignificant effectiveness for upper limb movement disorder both in the "on" and "off" medicine status (SMD = -0.07; 95% CI, -0.36 to 0.22; p = 0.64; I 2 = 0%; SMD = -0.21; 95% CI, -0.57 to 0.15; p = 0.26; I 2 = 0%; respectively). TBS significantly improved slowing of gait in the "off" medicine status (SMD = -0.37; 95% CI, -0.71 to -0.03; p = 0.03; I 2 = 0%). Subgroup analysis suggested that only intermittent TBS (iTBS) over the primary motor cortex (M1) + dorsolateral prefrontal cortex (DLPFC) had significant difference (SMD = -0.57; 95% CI, -1.13 to -0.01; p = 0.04). Additionally, iTBS over the M1+ DLPFC had a short-term (within 2 weeks) therapeutic effect on PD depression (MD = -2.93; 95% CI, -5.52 to -0.33; p = 0.03). Conclusion: Our study demonstrated that cTBS over the SMA could significantly improve the UPDRS-III score for PD patients in the "off," not in the "on," medicine state. TBS could not bring significant improvement of upper limb movement dysfunction. ITBS over the M1+DLPFC could significantly improve the slowing of gait in the "off" medicine status. Additionally, iTBS over the M1+DLPFC has a short-term (within 2 weeks) therapeutic effect on PD depression. Further RCTs of a large sample, and excellent design are needed to confirm our conclusions.
Keywords: Parkinson's disease; meta-analysis; non-invasive brain stimulation; repetitive transcranial magnetic stimulation; theta burst stimulation.
Copyright © 2022 Cheng, Zhu, Zhao, Sun, Shen, Xiao and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Twice-Daily Theta Burst Stimulation of the Dorsolateral Prefrontal Cortex Reduces Methamphetamine Craving: A Pilot Study.Front Neurosci. 2020 Mar 25;14:208. doi: 10.3389/fnins.2020.00208. eCollection 2020. Front Neurosci. 2020. PMID: 32273837 Free PMC article.
-
Repetitive transcranial magnetic stimulation therapy for motor recovery in Parkinson's disease: A Meta-analysis.Brain Behav. 2018 Nov;8(11):e01132. doi: 10.1002/brb3.1132. Epub 2018 Sep 28. Brain Behav. 2018. PMID: 30264518 Free PMC article.
-
Excitatory Repetitive Transcranial Magnetic Stimulation Over the Ipsilesional Hemisphere for Upper Limb Motor Function After Stroke: A Systematic Review and Meta-Analysis.Front Neurol. 2022 Jun 20;13:918597. doi: 10.3389/fneur.2022.918597. eCollection 2022. Front Neurol. 2022. PMID: 35795793 Free PMC article.
-
Treatment of major depressive disorder with bilateral theta burst stimulation: study protocol for a randomized, double-blind, placebo-controlled multicenter trial (TBS-D).Eur Arch Psychiatry Clin Neurosci. 2021 Oct;271(7):1231-1243. doi: 10.1007/s00406-021-01280-w. Epub 2021 Jun 19. Eur Arch Psychiatry Clin Neurosci. 2021. PMID: 34146143 Free PMC article.
-
Effects of Repetitive Transcranial Magnetic Stimulation on Motor Symptoms in Parkinson's Disease: A Meta-Analysis.Neurorehabil Neural Repair. 2022 Jul;36(7):395-404. doi: 10.1177/15459683221095034. Epub 2022 May 26. Neurorehabil Neural Repair. 2022. PMID: 35616427
Cited by
-
Noninvasive Neuromodulation in Parkinson's Disease: Insights from Animal Models.J Clin Med. 2023 Aug 22;12(17):5448. doi: 10.3390/jcm12175448. J Clin Med. 2023. PMID: 37685514 Free PMC article. Review.
-
Neuroprotective Effects of Intermittent Theta Burst Stimulation in Parkinson's Disease (NET-PD): A Study Protocol for a Delayed-Start Randomized Double-Blind Sham-Controlled Trial.J Clin Med. 2022 Aug 24;11(17):4972. doi: 10.3390/jcm11174972. J Clin Med. 2022. PMID: 36078903 Free PMC article.
-
Non-Pharmacological Interventions for Depression and Anxiety in Parkinson's Disease.J Parkinsons Dis. 2024;14(s1):S135-S146. doi: 10.3233/JPD-230228. J Parkinsons Dis. 2024. PMID: 38607762 Free PMC article. Review.
-
[Research progress on repetitive transcranial magnetic stimulation for improving depression in Parkinson's disease].Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2025 Apr 25;42(2):404-408. doi: 10.7507/1001-5515.202410040. Sheng Wu Yi Xue Gong Cheng Xue Za Zhi. 2025. PMID: 40288985 Free PMC article. Review. Chinese.
-
The effects of transcranial magnetic stimulation in motor symptoms of Parkinson's disease: an overview of systematic reviews with meta-analysis.Neurol Sci. 2025 Aug;46(8):3405-3418. doi: 10.1007/s10072-025-08189-5. Epub 2025 Apr 16. Neurol Sci. 2025. PMID: 40237970 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous