

Management of proximal biceps tendon pathology
- PMID: 35096535
- PMCID: PMC8771414
- DOI: 10.5312/wjo.v13.i1.36
Management of proximal biceps tendon pathology
Abstract
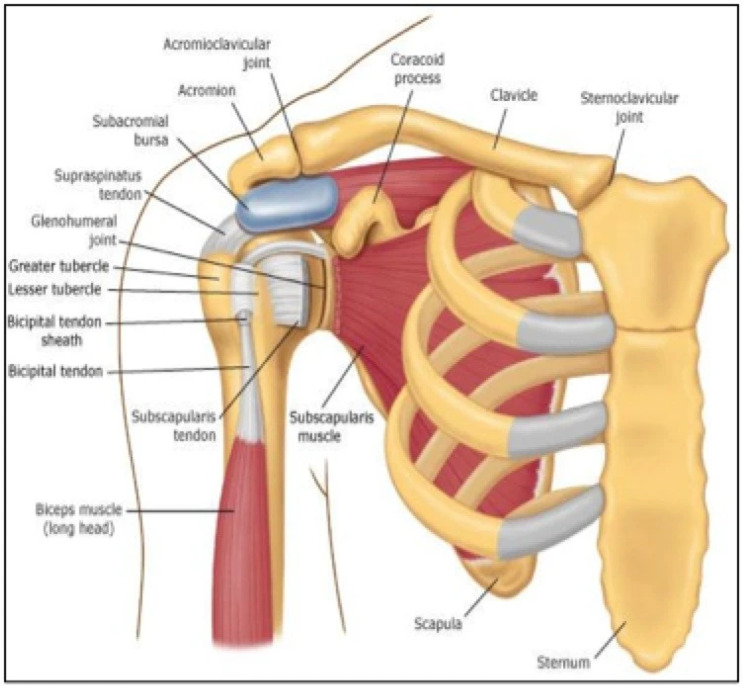
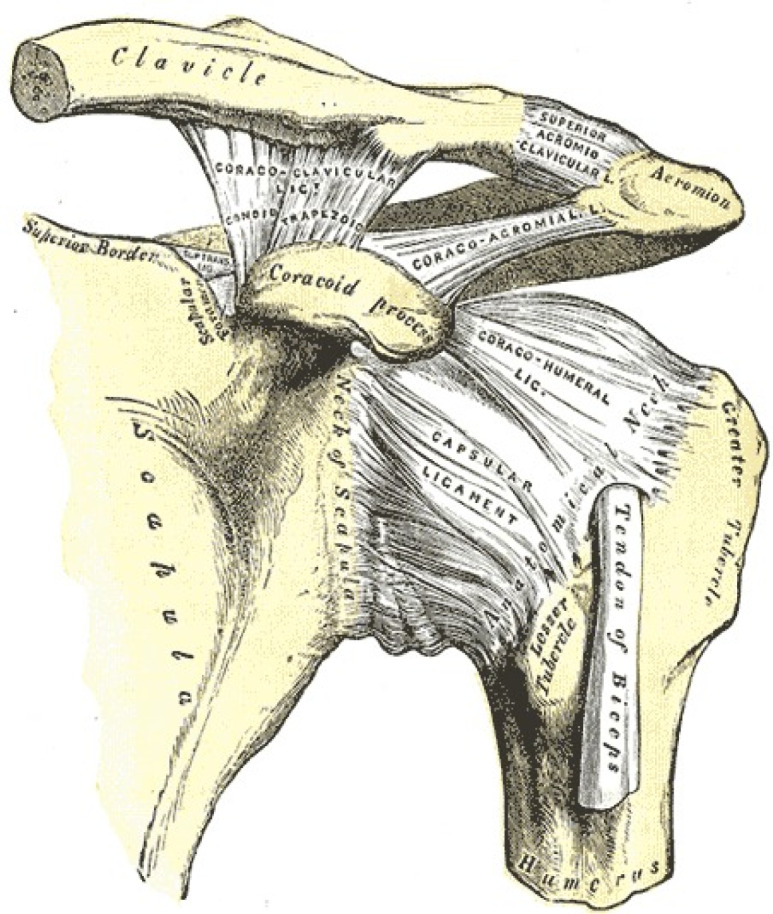
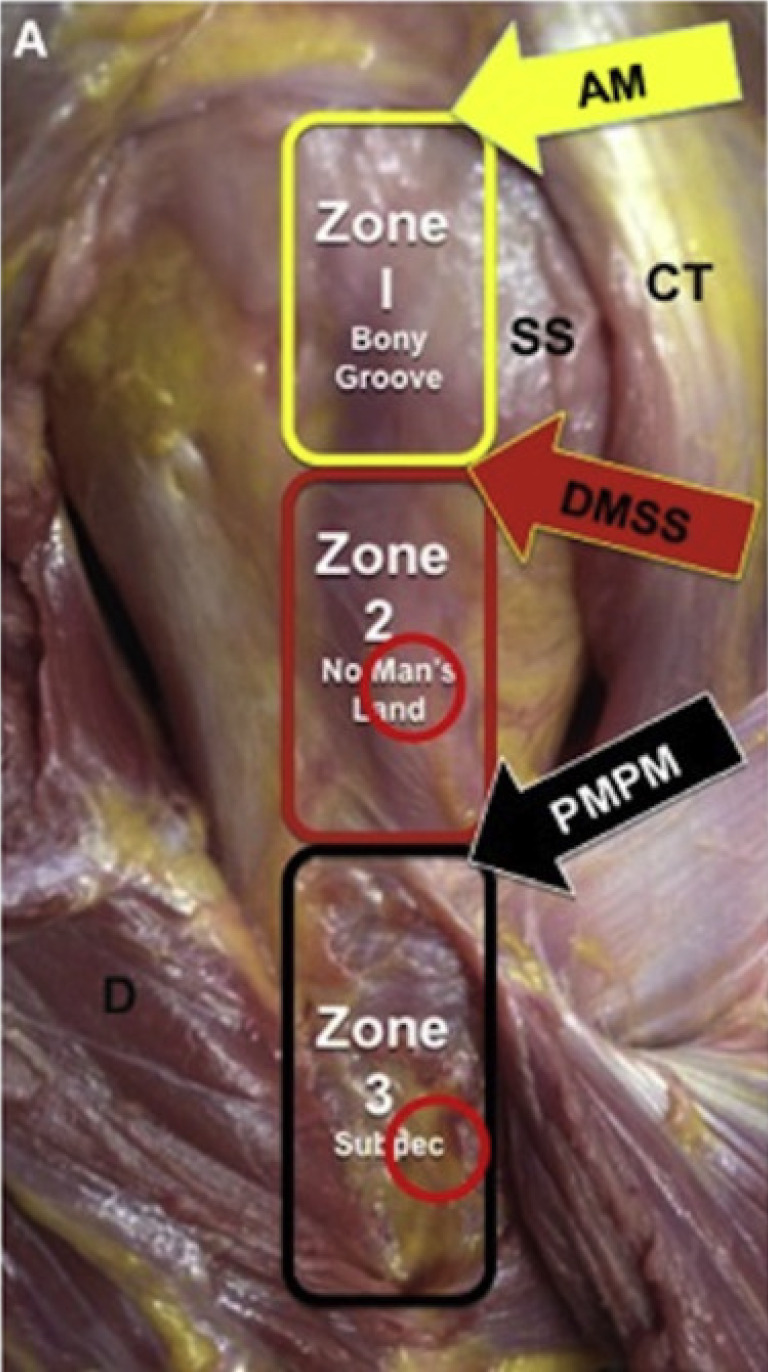
The long head of the biceps tendon is widely recognized as an important pain generator, especially in anterior shoulder pain and dysfunction with athletes and working individuals. The purpose of this review is to provide a current understanding of the long head of the biceps tendon anatomy and its surrounding structures, function, and relevant clinical information such as evaluation, treatment options, and complications in hopes of helping orthopaedic surgeons counsel their patients. An understanding of the long head of the biceps tendon anatomy and its surrounding structures is helpful to determine normal function as well as pathologic injuries that stem proximally. The biceps-labral complex has been identified and broken down into different regions that can further enhance a physician's knowledge of common anterior shoulder pain etiologies. Although various physical examination maneuvers exist meant to localize the anterior shoulder pain, the lack of specificity requires orthopaedic surgeons to rely on patient history, advanced imaging, and diagnostic injections in order to determine the patient's next steps. Nonsurgical treatment options such as anti-inflammatory medications, physical therapy, and ultrasound-guided corticosteroid injections should be utilized before entertaining surgical treatment options. If surgery is needed, the three options include biceps tenotomy, biceps tenodesis, or superior labrum anterior to posterior repair. Specifically for biceps tenodesis, recent studies have analyzed open vs arthroscopic techniques, the ideal location of tenodesis with intra-articular, suprapectoral, subpectoral, extra-articular top of groove, and extra-articular bottom of groove approaches, and the best method of fixation using interference screws, suture anchors, or cortical buttons. Orthopaedic surgeons should be aware of the complications of each procedure and respond accordingly for each patient. Once treated, patients often have good to excellent clinical outcomes and low rates of complications.
Keywords: Biceps tenodesis; Biceps tenotomy; Biceps-labral complex; Long head of the biceps tendon; Shoulder pathology; Superior labrum anterior to posterior lesions.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Simon P Lalehzarian, Avinesh Agarwalla, and Joseph N Liu have no conflicts of interest to report.
Figures




References
-
- Boileau P, Parratte S, Chuinard C, Roussanne Y, Shia D, Bicknell R. Arthroscopic treatment of isolated type II SLAP lesions: biceps tenodesis as an alternative to reinsertion. Am J Sports Med. 2009;37:929–936. - PubMed
-
- Denard PJ, Lädermann A, Parsley BK, Burkhart SS. Arthroscopic biceps tenodesis compared with repair of isolated type II SLAP lesions in patients older than 35 years. Orthopedics. 2014;37:e292–e297. - PubMed
-
- Ek ET, Shi LL, Tompson JD, Freehill MT, Warner JJ. Surgical treatment of isolated type II superior labrum anterior-posterior (SLAP) lesions: repair versus biceps tenodesis. J Shoulder Elbow Surg. 2014;23:1059–1065. - PubMed
-
- Patterson BM, Creighton RA, Spang JT, Roberson JR, Kamath GV. Surgical Trends in the Treatment of Superior Labrum Anterior and Posterior Lesions of the Shoulder: Analysis of Data From the American Board of Orthopaedic Surgery Certification Examination Database. Am J Sports Med. 2014;42:1904–1910. - PubMed
-
- Krupp RJ, Kevern MA, Gaines MD, Kotara S, Singleton SB. Long head of the biceps tendon pain: differential diagnosis and treatment. J Orthop Sports Phys Ther. 2009;39:55–70. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
